

Low-gradient aortic stenosis
- PMID: 27190103
- PMCID: PMC5030681
- DOI: 10.1093/eurheartj/ehw096
Low-gradient aortic stenosis
Abstract
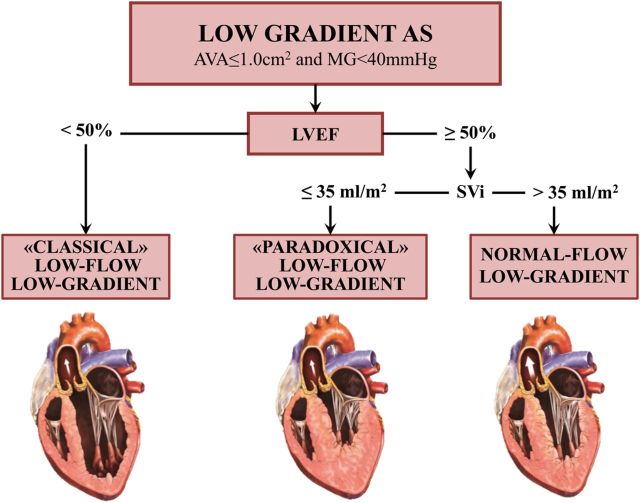
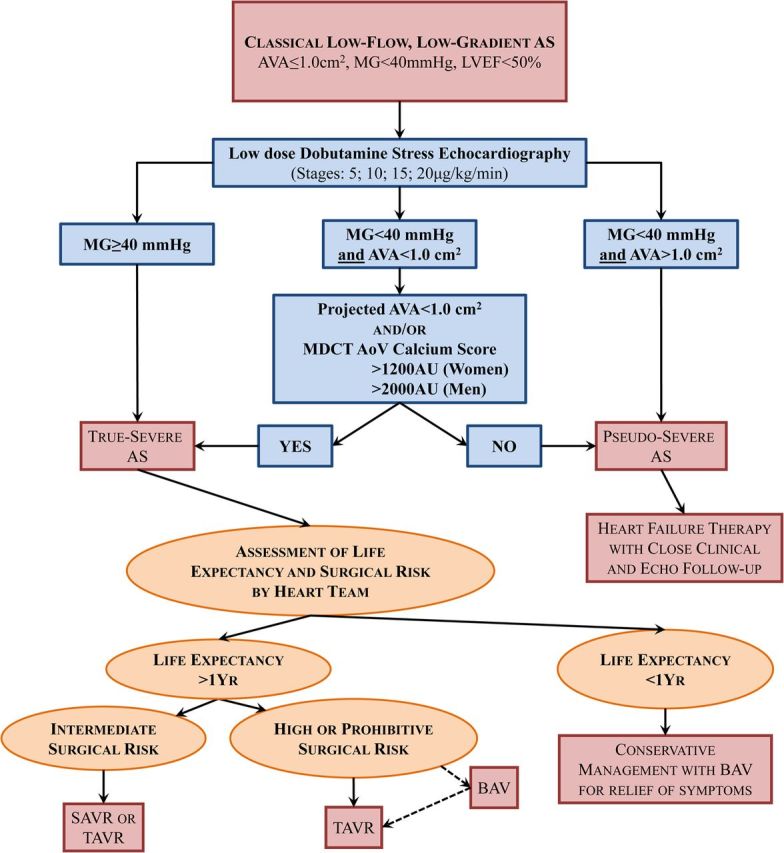
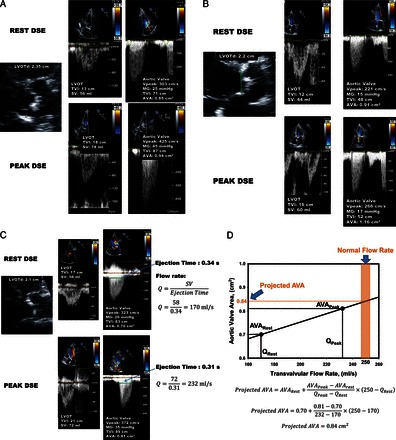
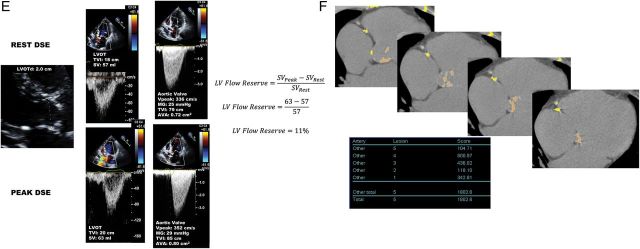
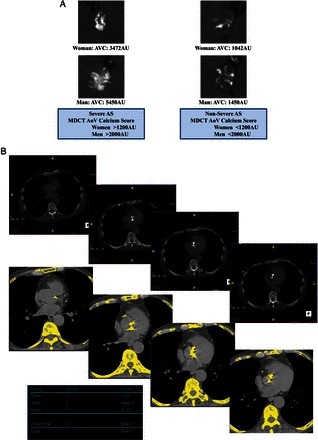
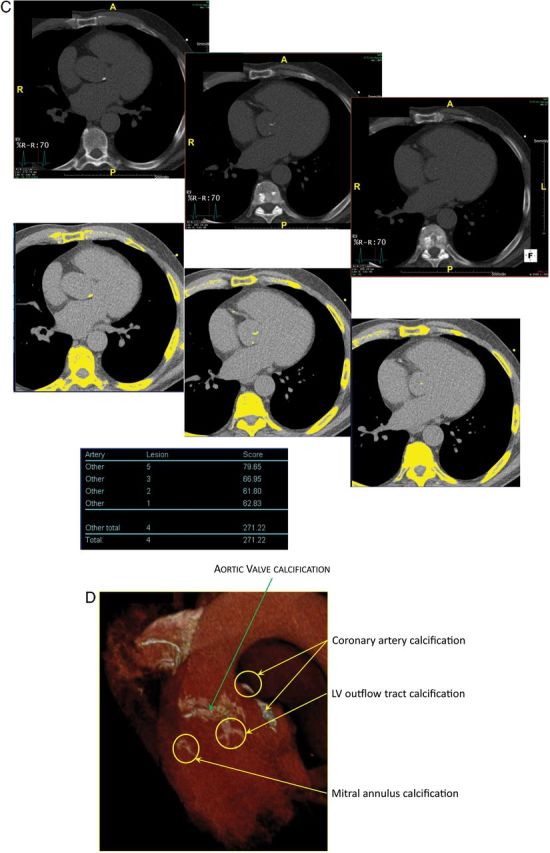
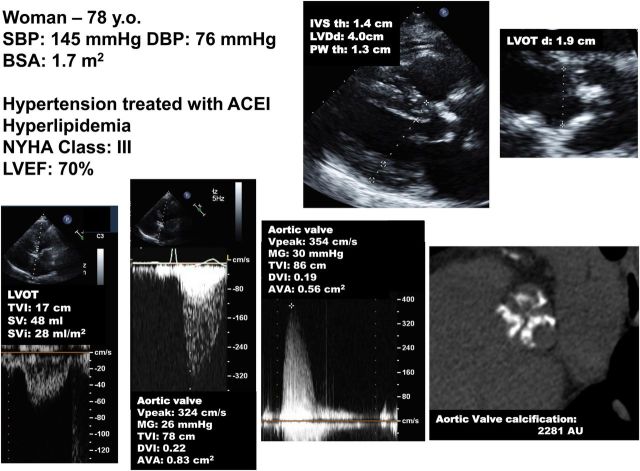
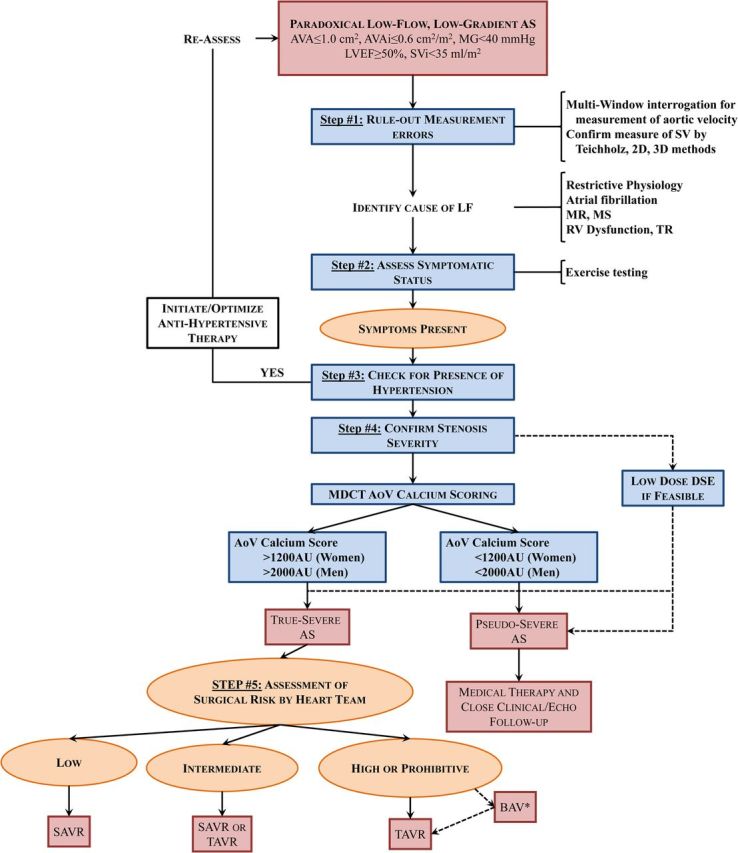
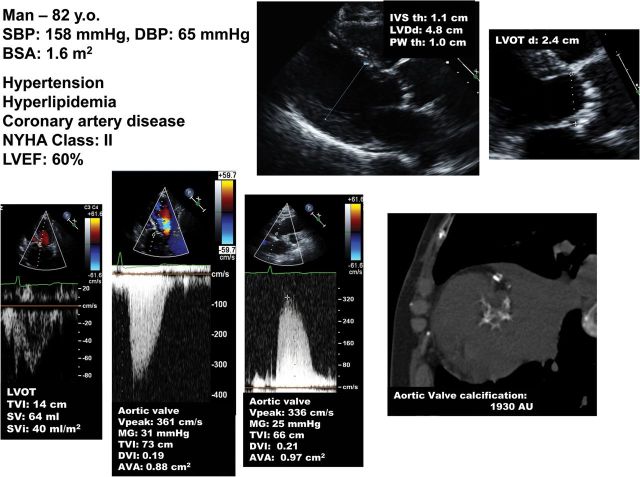
An important proportion of patients with aortic stenosis (AS) have a 'low-gradient' AS, i.e. a small aortic valve area (AVA <1.0 cm(2)) consistent with severe AS but a low mean transvalvular gradient (<40 mmHg) consistent with non-severe AS. The management of this subset of patients is particularly challenging because the AVA-gradient discrepancy raises uncertainty about the actual stenosis severity and thus about the indication for aortic valve replacement (AVR) if the patient has symptoms and/or left ventricular (LV) systolic dysfunction. The most frequent cause of low-gradient (LG) AS is the presence of a low LV outflow state, which may occur with reduced left ventricular ejection fraction (LVEF), i.e. classical low-flow, low-gradient (LF-LG), or preserved LVEF, i.e. paradoxical LF-LG. Furthermore, a substantial proportion of patients with AS may have a normal-flow, low-gradient (NF-LG) AS: i.e. a small AVA-low-gradient combination but with a normal flow. One of the most important clinical challenges in these three categories of patients with LG AS (classical LF-LG, paradoxical LF-LG, and NF-LG) is to differentiate a true-severe AS that generally benefits from AVR vs. a pseudo-severe AS that should be managed conservatively. A low-dose dobutamine stress echocardiography may be used for this purpose in patients with classical LF-LG AS, whereas aortic valve calcium scoring by multi-detector computed tomography is the preferred modality in those with paradoxical LF-LG or NF-LG AS. Although patients with LF-LG severe AS have worse outcomes than those with high-gradient AS following AVR, they nonetheless display an important survival benefit with this intervention. Some studies suggest that transcatheter AVR may be superior to surgical AVR in patients with LF-LG AS.
Keywords: Aortic stenosis; Aortic valve replacement; Computed tomography; Echocardiography; Low flow; Low gradient; Transcatheter aortic valve replacement.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
TAVI for patients with normal-flow low-gradient compared to high-gradient aortic stenosis.Int J Cardiol. 2023 Jan 15;371:299-304. doi: 10.1016/j.ijcard.2022.10.143. Epub 2022 Oct 25. Int J Cardiol. 2023. PMID: 36306951
References
-
- Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De BM, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schafers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, von Oppell UO, Windecker S, Zamorano JL, Zembala M. Guidelines on the management of valvular heart disease (version 2012). Joint task force on the management of valvular heart disease of the European Society of Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2012;33:2451–2496. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM, Thomas JD. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary. A report of the American College of Cardiology/American heart association task force on practice guidelines. J Am Coll Cardiol 2014;63:2438–2488. - PubMed
-
- Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low flow, low gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation 2007;115:2856–2864. - PubMed
-
- Minners J, Allgeier M, Gohlke-Baerwolf C, Kienzle RP, Neumann FJ, Jander N. Inconsistent grading of aortic valve stenosis by current guidelines: haemodynamic studies in patients with apparently normal left ventricular function. Heart 2010;96:1463–1468. - PubMed
-
- Lancellotti P, Magne J, Donal E, Davin L, O'Connor K, Rosca M, Szymanski C, Cosyns B, Piérard LA. Clinical outcome in asymptomatic severe aortic stenosis. Insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol 2012;59:235–243. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
