

Baseline Inflammatory Biomarkers Identify Subgroups of HIV-Infected African Children With Differing Responses to Antiretroviral Therapy
- PMID: 27190179
- PMCID: PMC4918830
- DOI: 10.1093/infdis/jiw148
Baseline Inflammatory Biomarkers Identify Subgroups of HIV-Infected African Children With Differing Responses to Antiretroviral Therapy
Abstract
Background: Identifying determinants of morbidity and mortality may help target future interventions for human immunodeficiency virus (HIV)-infected children.
Methods: CD4(+) T-cell count, HIV viral load, and levels of biomarkers (C-reactive protein, tumor necrosis factor α [TNF-α], interleukin 6 [IL-6], and soluble CD14) and interleukin 7 were measured at antiretroviral therapy (ART) initiation in the ARROW trial (case-cohort design). Cases were individuals who died, had new or recurrent World Health Organization clinical stage 4 events, or had poor immunological response to ART.
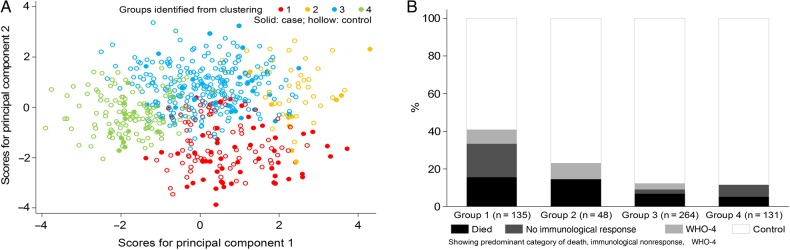
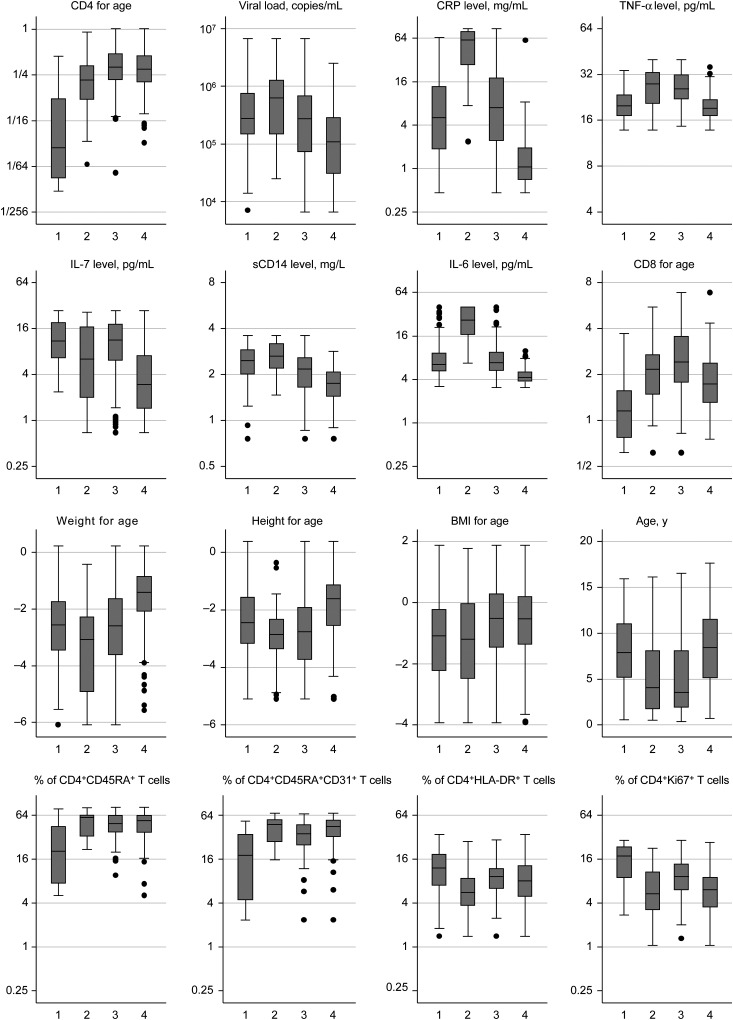
Results: There were 115 cases (54 died, 45 had World Health Organization clinical stage 4 events, and 49 had poor immunological response) and 485 controls. Before ART initiation, the median ages of cases and controls were 8.2 years (interquartile range [IQR], 4.4-11.4 years) and 5.8 years (IQR, 2.3-9.3 years), respectively, and the median percentages of lymphocytes expressing CD4 were 4% (IQR, 1%-9%) and 13% (IQR, 8%-18%), respectively. In multivariable logistic regression, cases had lower age-associated CD4(+) T-cell count ratio (calculated as the ratio of the subject's CD4(+) T-cell count to the count expected in healthy individuals of the same age; P < .0001) and higher IL-6 level (P = .002) than controls. Clustering biomarkers and age-associated CD4(+) and CD8(+) T-cell count ratios identified 4 groups of children. Group 1 had the highest frequency of cases (41% cases; 16% died) and profound immunosuppression; group 2 had similar mortality (23% cases; 15% died), but children were younger, with less profound immunosuppression and high levels of inflammatory biomarkers and malnutrition; group 3 comprised young children with moderate immunosuppression, high TNF-α levels, and high age-associated CD8(+) T-cell count ratios but lower frequencies of events (12% cases; 7% died); and group 4 comprised older children with low inflammatory biomarker levels, lower HIV viral loads, and good clinical outcomes (11% cases; 5% died).
Conclusions: While immunosuppression is the major determinant of poor outcomes during ART, baseline inflammation is an additional important factor, identifying a subgroup of young children with similar mortality. Antiinflammatory interventions may help improve outcomes.
Keywords: Africa; HIV; children; immunosuppression; inflammation.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Health Organization (WHO). Global update on the health sector response to HIV, executive summary. Geneva: WHO, 2014. http://www.who.int/hiv/pub/progressreports/update2014-executive-summary/en/ Accessed 31 July 2014.
-
- UNAIDS. The gap report. Geneva: UNAIDS, 2014. http://www.unaids.org/en/resources/documents/2014 Accessed 22 November 2015.
-
- Nugent J, Edmonds A, Lusiama J et al. Predicting mortality in HIV-infected children initiating highly active antiretroviral therapy in a resource-deprived setting. Pediatr Infect Dis J 2014; 33:1148–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
