

The imaging of osteomyelitis
- PMID: 27190771
- PMCID: PMC4858469
- DOI: 10.21037/qims.2016.04.01
The imaging of osteomyelitis
Abstract
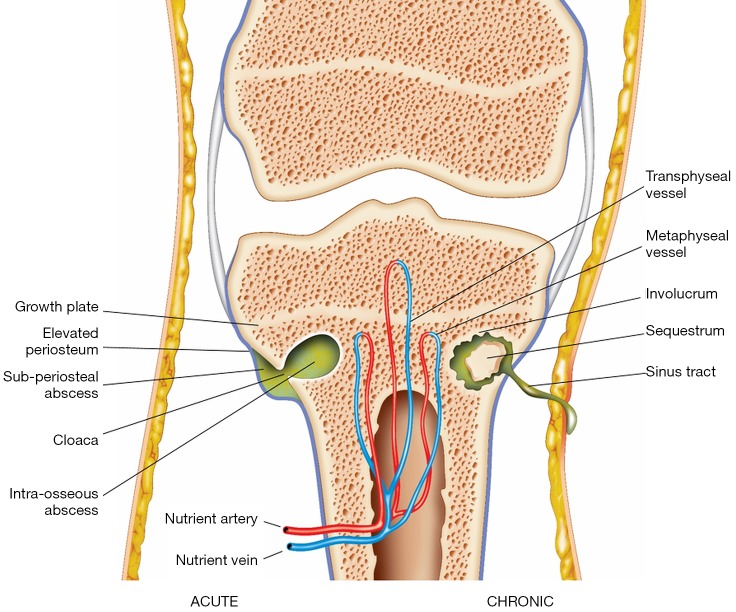
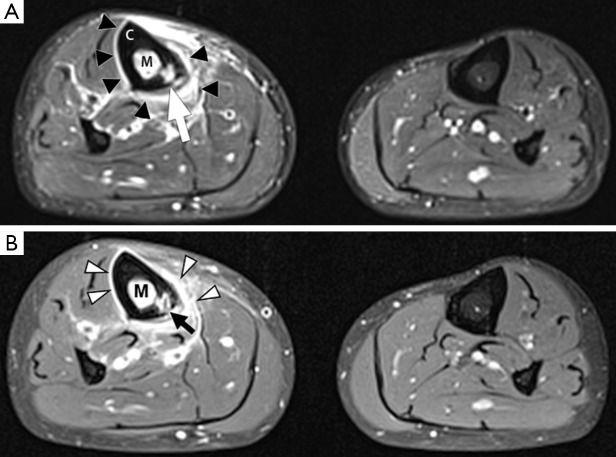
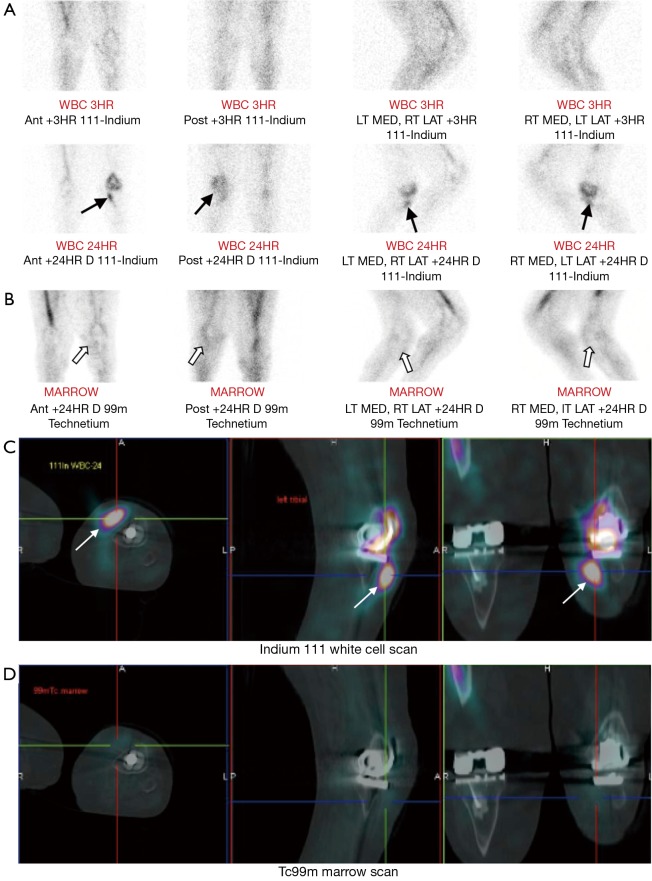
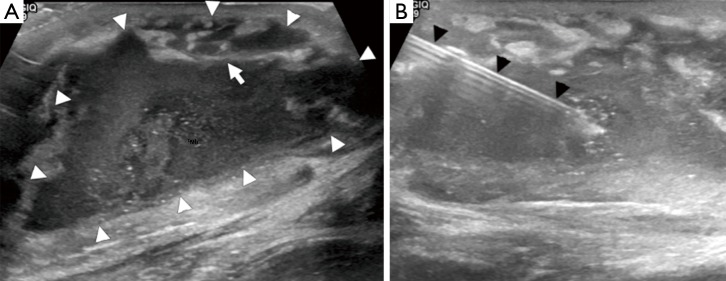
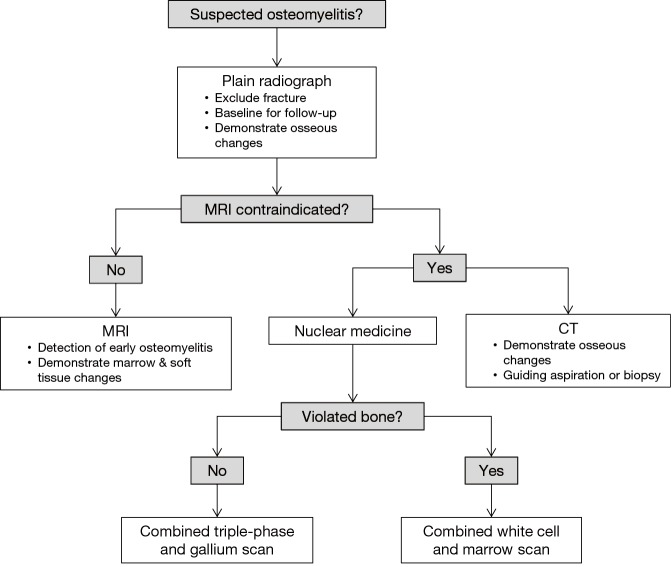
Osteomyelitis is an important cause of morbidity and mortality in children and adults. Imaging plays a crucial role in establishing a timely diagnosis and guiding early management, with the aim of reducing long-term complications. Recognition of the imaging features of osteomyelitis requires a good understanding of its pathogenesis. In this review, the key imaging findings in osteomyelitis are correlated with the underlying pathological processes. There is a particular emphasis on magnetic resonance imaging (MRI), which is the best available imaging modality owing to its high sensitivity for detecting early osteomyelitis, excellent anatomical detail and superior soft tissue resolution. However, other modalities such as nuclear medicine and computed tomography (CT) are also useful in many clinical contexts, and will also be described in this review.
Keywords: Musculoskeletal; infection; magnetic resonance imaging (MRI); radiology.
Conflict of interest statement
Figures




References
-
- Arnold SR, Elias D, Buckingham SC, Thomas ED, Novais E, Arkader A, Howard C. Changing patterns of acute hematogenous osteomyelitis and septic arthritis: emergence of community-associated methicillin-resistant Staphylococcus aureus. J Pediatr Orthop 2006;26:703-8. 10.1097/01.bpo.0000242431.91489.b4 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources