

Cost-Effectiveness Analysis of Screening for and Managing Identified Hypertension for Cardiovascular Disease Prevention in Vietnam
- PMID: 27192051
- PMCID: PMC4871542
- DOI: 10.1371/journal.pone.0155699
Cost-Effectiveness Analysis of Screening for and Managing Identified Hypertension for Cardiovascular Disease Prevention in Vietnam
Abstract
Objective: To inform development of guidelines for hypertension management in Vietnam, we evaluated the cost-effectiveness of different strategies on screening for hypertension in preventing cardiovascular disease (CVD).
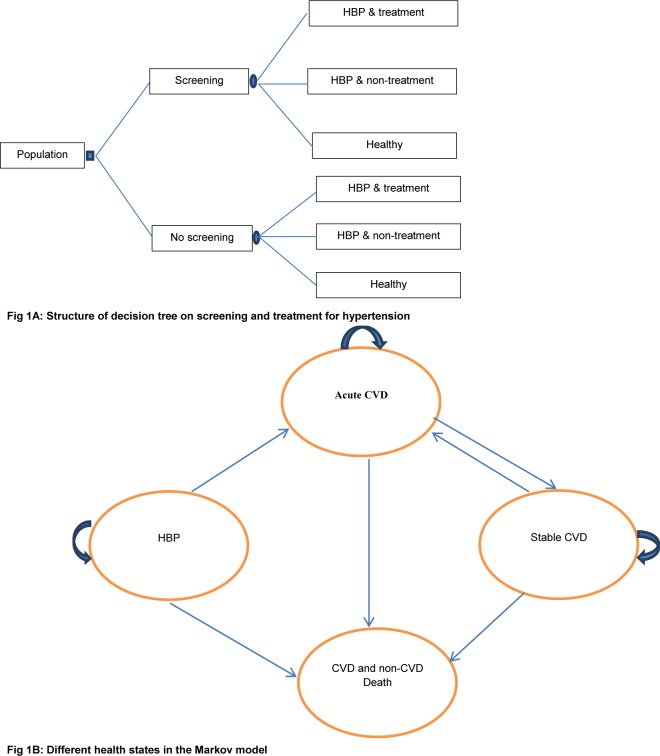
Methods: A decision tree was combined with a Markov model to measure incremental cost-effectiveness of different approaches to hypertension screening. Values used as input parameters for the model were taken from different sources. Various screening intervals (one-off, annually, biannually) and starting ages to screen (35, 45 or 55 years) and coverage of treatment were analysed. We ran both a ten-year and a lifetime horizon. Input parameters for the models were extracted from local and regional data. Probabilistic sensitivity analysis was used to evaluate parameter uncertainty. A threshold of three times GDP per capita was applied.
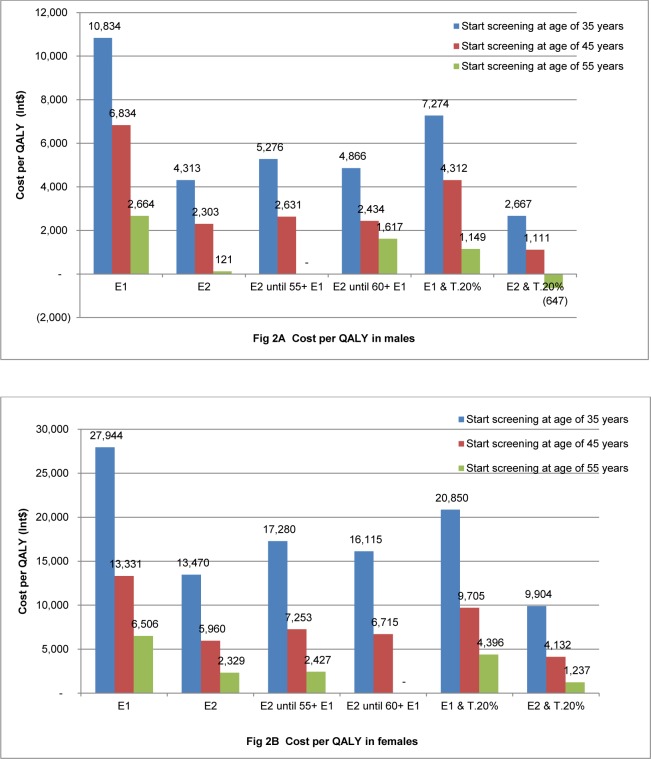
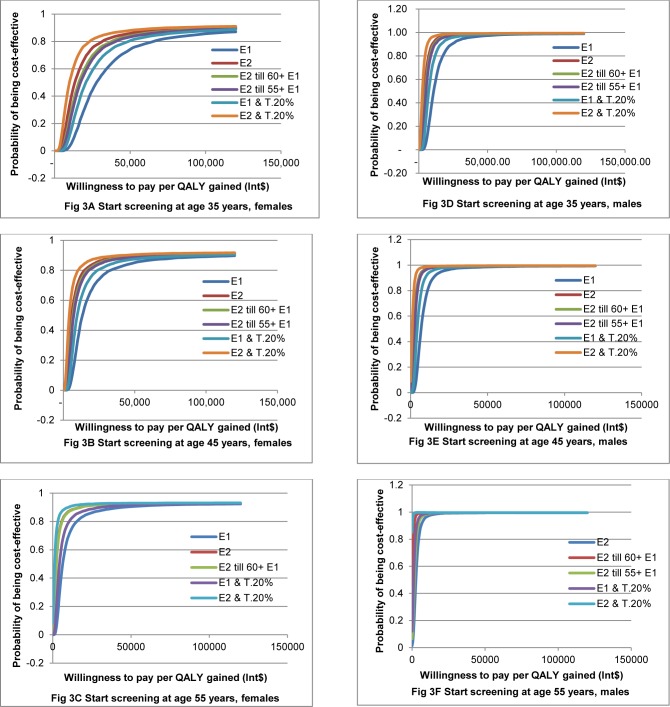
Results: Cost per quality adjusted life year (QALY) gained varied in different screening scenarios. In a ten-year horizon, the cost-effectiveness of screening for hypertension ranged from cost saving to Int$ 758,695 per QALY gained. For screening of men starting at 55 years, all screening scenarios gave a high probability of being cost-effective. For screening of females starting at 55 years, the probability of favourable cost-effectiveness was 90% with one-off screening. In a lifetime horizon, cost per QALY gained was lower than the threshold of Int$ 15,883 in all screening scenarios among males. Similar results were found in females when starting screening at 55 years. Starting screening in females at 45 years had a high probability of being cost-effective if screening biannually was combined with increasing coverage of treatment by 20% or even if sole biannual screening was considered.
Conclusion: From a health economic perspective, integrating screening for hypertension into routine medical examination and related coverage by health insurance could be recommended. Screening for hypertension has a high probability of being cost-effective in preventing CVD. An adequate screening strategy can best be selected based on age, sex and screening interval.
Conflict of interest statement
Figures
References
-
- World Health Organization. (2013). A global brief on hypertension. Available: http://apps.who.int/iris/bitstream/10665/79059/1/WHO_DCO_WHD_2013.2_eng.....
-
- Institute for Health Metrics and Evaluation. (2016) Global Burden of Disease. Available: http://vizhub.healthdata.org/gbd-compare/.
-
- Yano Y, Briasoulis A, Bakris GL, Hoshide S, Wang JG, et al. (2014) Effects of antihypertensive treatment in Asian populations: a meta-analysis of prospective randomized controlled studies (CARdiovascular protectioN group in Asia: CARNA). J Am Soc Hypertens 8: 103–116. 10.1016/j.jash.2013.09.002 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
