

doi: 10.1007/s13244-016-0500-y.
Epub 2016 May 18.
Atraumatic splenic rupture, an underrated cause of acute abdomen
Affiliations
- PMID: 27193528
- PMCID: PMC4956628
- DOI: 10.1007/s13244-016-0500-y
Item in Clipboard
Atraumatic splenic rupture, an underrated cause of acute abdomen
Insights Imaging.
2016 Aug.
Erratum in
-
Erratum to: Atraumatic splenic rupture, an underrated cause of acute abdomen.Insights Imaging. 2016 Aug;7(4):647. doi: 10.1007/s13244-016-0508-3. Insights Imaging. 2016. PMID: 27357397 Free PMC article. No abstract available.
No abstract available
Figures
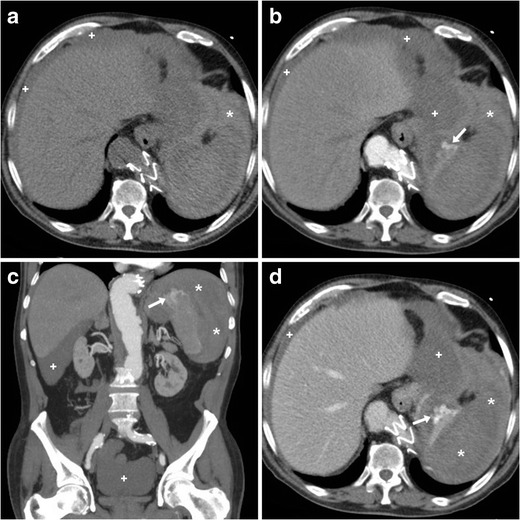
A 75-year-old male presented to emergency department with generalised acute abdominal pain and physical signs of haemodynamic impairment. His past medical history included coronary stenting and endovascular treatment of aneurysmal dilatation of the thoracic aorta, respectively, 13 and 5 years earlier. He denied trauma and unusual efforts, and was on regular warfarin anticoagulation. Bedside ultrasound (not shown) revealed echogenic peritoneal effusion. Emergency multidetector CT including unenhanced (a), arterial- (b, c), and portal venous (D) post-contrast acquisitions showed a normal-sized spleen, compressed by the extensive perisplenic haemorrhage (*). Contrast extravasation isoattenuating with enhanced blood vessels (arrows in B…D) and increasing from the arterial to the venous acquisition was noted at the upper splenic pole, indicating non-contained active bleeding. Multi-compartmental haemoperitoneum (+) was present. Note the metallic endoprosthesis of the distal thoracic descending aorta. Immediate splenectomy confirmed bleeding from a polar laceration. Gross and microscopic pathology did not disclose underlying abnormalities
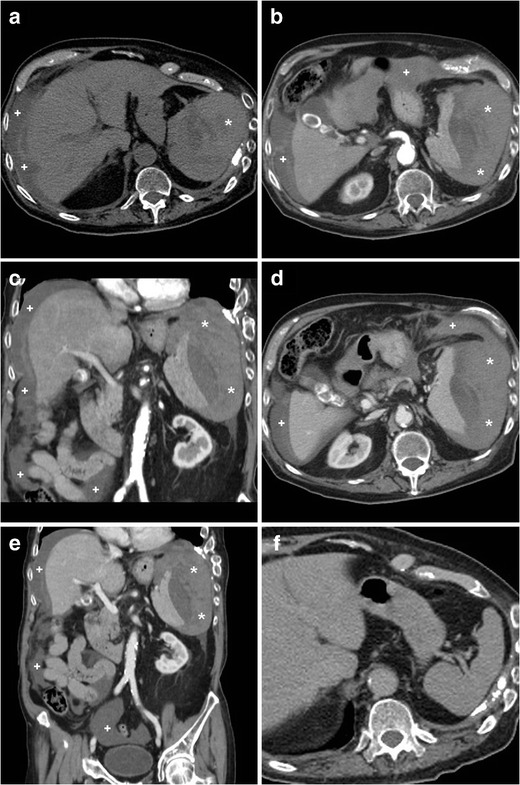
An elderly 89-year-old male with chronic heart failure, previous transurethral resection of non-muscle-invasive urinary bladder carcinoma, and lung emphysema experienced sudden hypotension and fainting. He was not on anticoagulants. Physical findings included palpation tenderness in the left hemiabdomen, tachycardia, and hypotension. Laboratory tests revealed severe blood loss: haemoglobin dropped from 9.2 to 6.4 g/dl within four hours. Platelet count, prothrombin time, and activated partial thromboplastin time were within normal range. Urgent CT including unenhanced (a), arterial- (b, c) and venous-phase (d, e) post-contrast images revealed mixed attenuation peritoneal effusion (+) consistent with haemoperitoneum. The spleen was surrounded, medially dislocated, and compressed by massive, fresh hyperattenuating (up to 55 Hounsfield units), partly subcapsular haemorrhage (*). Pseudoaneurysms and active bleeding were not seen. The spleen showed homogeneous parenchymal enhancement without focal lesions or signs of diffuse infiltrating disease. Retrospectively, contrast-enhanced CT obtained four months earlier (F) for bladder cancer staging revealed a normal, homogeneous spleen. The patient underwent urgent splenectomy and eventually recovered. Surgical pathology revealed medium-sized spleen with reactive lymphoid hyperplasia, and excluded acute infectious or neoplastic changes. Final diagnosis was idiopathic splenic rupture
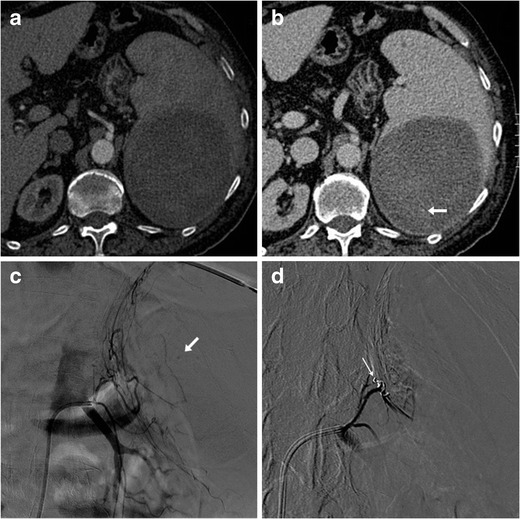
A 73-year-old male on anticoagulation suffered from spontaneous acute abdominal pain. His medical history included congestive heart failure, complete atrioventricular block treated with an implantable cardioverter-defibrillator, previous angioplasty and coronary stenting for acute myocardial infarction, and surgically treated colon carcinoma. Physical examination revealed hypotension and tender left hypocondrium. The international normalized ratio (INR) was 2.6; haemoglobin level was 6.5 g/dl. CT (a, b) revealed a large, roundish mixed attenuation intraparenchymal splenic haematoma without haemoperitoneum. Active bleeding was not evident during the arterial-phase acquisition (a). Faint contrast “blush” (arrow in b) was visible in the venous phase and confirmed at urgent arteriography as minimal bleeding originating from the left phrenic artery (arrow in c). Selective embolization with Spongostan and coil (thin arrow in d) was performed and allowed successful nonoperative management
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
