

The availability of emergency obstetric care in the context of the JSY cash transfer programme in Madhya Pradesh, India
- PMID: 27193837
- PMCID: PMC4872340
- DOI: 10.1186/s12884-016-0896-x
The availability of emergency obstetric care in the context of the JSY cash transfer programme in Madhya Pradesh, India
Abstract
Background: Since 2005, India has implemented a national cash transfer programme, the Janani Suraksha Yojana (JSY), which provides women a cash transfer upon giving birth in an existing public facility. This has resulted in a steep rise in facility births across the country. The early years of the programme saw efforts being made to strengthen the ability of facilities to provide obstetric care. Given that the JSY has been able to draw millions of women into facilities to give birth (there have been more than 50 million beneficiaries thus far), it is important to study the ability of these facilities to provide emergency obstetric care (EmOC), as the functionality of these facilities is critical to improved maternal and neonatal outcomes. We studied the availability and level of provision of EmOC signal functions in public facilities implementing the JSY programme in three districts of Madhya Pradesh (MP) state, central India. These are measured against the World Health Report (WHR) 2005benchmarks. As a comparison, we also study the functionality and contribution of private sector facilities to the provision of EmOC in these districts.
Methods: A cross-sectional survey of all healthcare facilities offering intrapartum care was conducted between February 2012 and April 2013. The EmOC signal functions performed in each facility were recorded, as were human resource data and birth numbers for each facility.
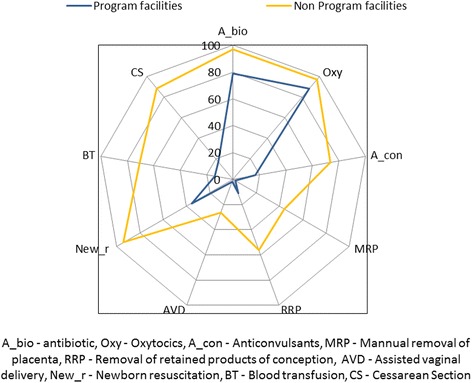
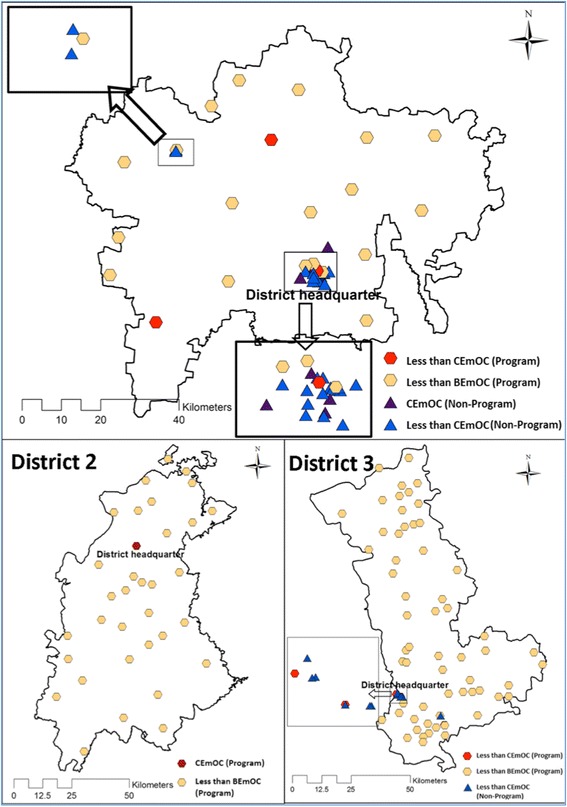
Results: A total of 152 facilities were surveyed of which 118 were JSY programme facilities. Eighty-six percent of childbirths occurred at programme facilities, two thirds of which occurred at facilities that did not meet standards for the provision basic emergency obstetric care. Of the 29 facilities that could perform caesareans, none could perform all the basic EmOC functions. Programme facilities provided few EmOC signal functions apart from parenteral antibiotic or oxytocic administration. Complicated EmOC provision was found predominantly in non-programme (private) facilities; only one of six facilities able to provide such care was in the public sector and therefore in the JSY programme. Only 13 % of all qualified obstetricians practiced at programme facilities.
Conclusions: Given the high proportion of births in public facilities in the state, the JSY programme has an opportunity to contribute to the reduction in maternal and perinatal mortality However, for the programme to have a greater impact on outcomes; EmOC provision must be significantly improved.. While private, non-programme facilities have better human resources and perform caesareans, most women in the state give birth under the JSY programme in the public sector. A demand-side programme such as the JSY will only be effective alongside an adequate supply side (i.e., a facility able to provide EmOC).
Figures
References
-
- Rai RK, Tulchinsky TH. Addressing the Sluggish Progress in Reducing Maternal Mortality in India. Asia Pac J Public Health. 2012; 27(2):1161-69. DOI:10.1177/1010539512436883. - PubMed
-
- WHO . Trends in Maternal Mortality: 1990 to 2013. Geneva: World Health Organization; 2014.
-
- Ministry of Health and Family Welfare Reproductive and Child Health programme (RCH) II . Document 2. The Principles and Evidence Base for State RCH II Programme Implementation Plan (PIPs) New Delhi: Government of India; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
