

Final results of the second prospective AIEOP protocol for pediatric intracranial ependymoma
- PMID: 27194148
- PMCID: PMC5035526
- DOI: 10.1093/neuonc/now108
Final results of the second prospective AIEOP protocol for pediatric intracranial ependymoma
Abstract
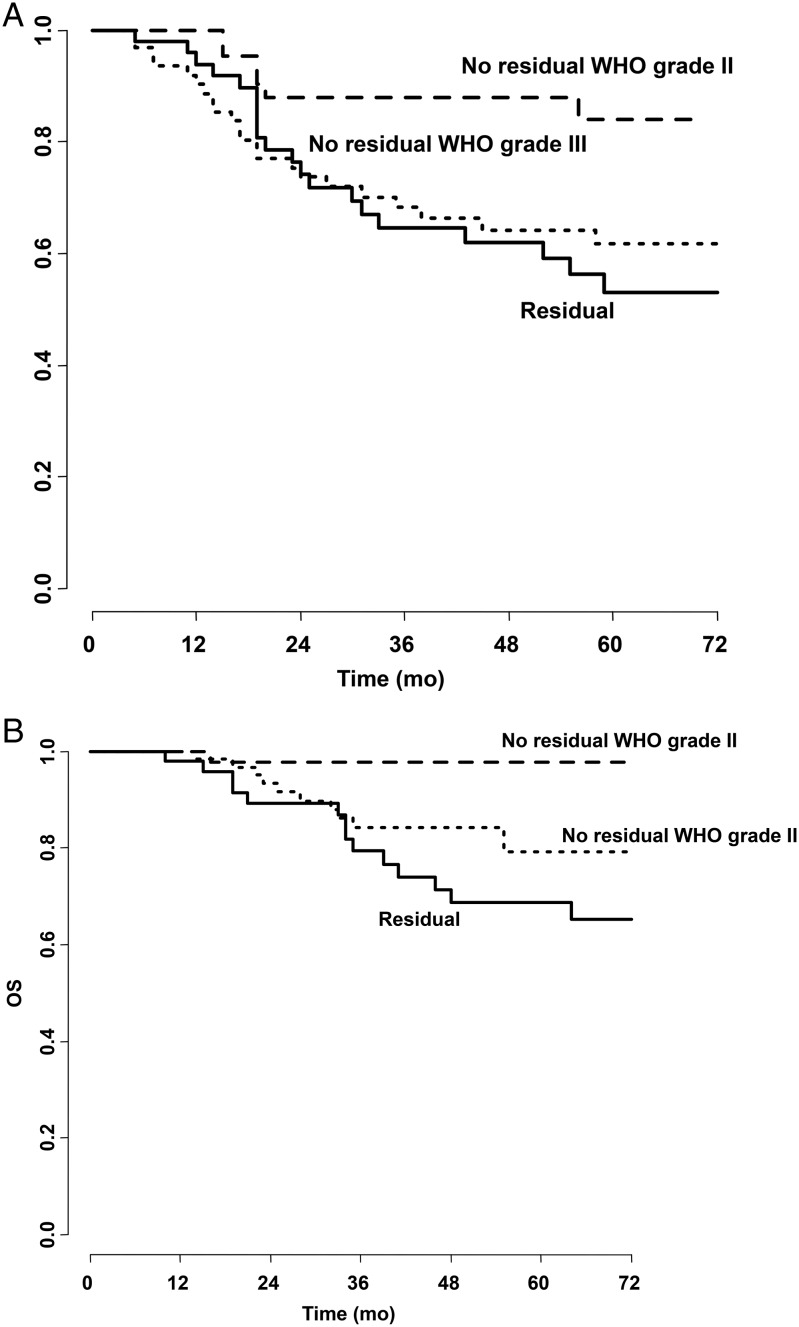
Background: This prospective study stratified patients by surgical resection (complete = NED vs incomplete = ED) and centrally reviewed histology (World Health Organization [WHO] grade II vs III).
Methods: WHO grade II/NED patients received focal radiotherapy (RT) up to 59.4 Gy with 1.8 Gy/day. Grade III/NED received 4 courses of VEC (vincristine, etoposide, cyclophosphamide) after RT. ED patients received 1-4 VEC courses, second-look surgery, and 59.4 Gy followed by an 8-Gy boost in 2 fractions on still measurable residue. NED children aged 1-3 years with grade II tumors could receive 6 VEC courses alone.
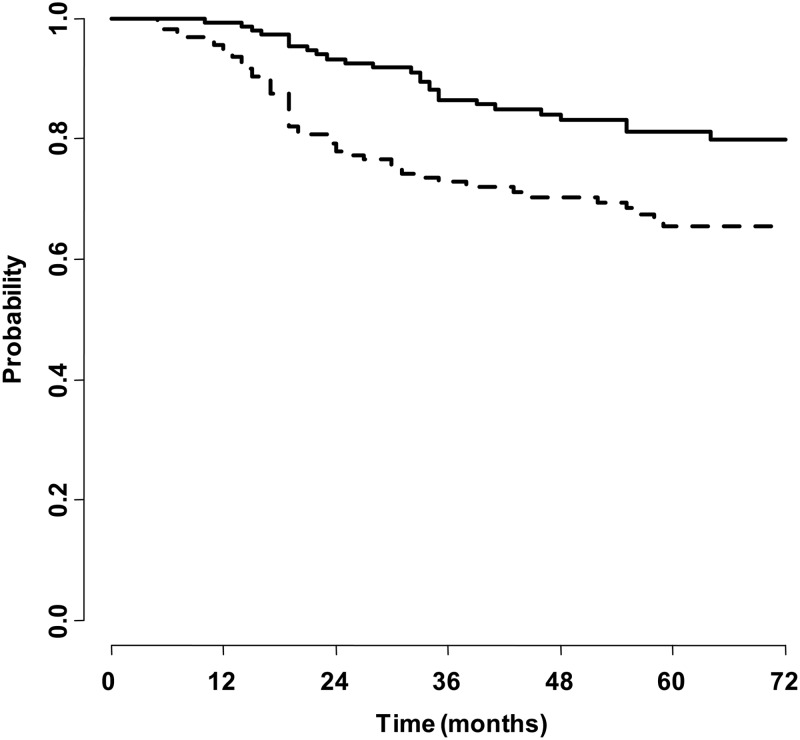
Results: From January 2002 to December 2014, one hundred sixty consecutive children entered the protocol (median age, 4.9 y; males, 100). Follow-up was a median of 67 months. An infratentorial origin was identified in 110 cases. After surgery, 110 patients were NED, and 84 had grade III disease. Multiple resections were performed in 46/160 children (28.8%). A boost was given to 24/40 ED patients achieving progression-free survival (PFS) and overall survival (OS) rates of 58.1% and 68.7%, respectively, in this poor prognosis subgroup. For the whole series, 5-year PFS and OS rates were 65.4% and 81.1%, with no toxic deaths. On multivariable analysis, NED status and grade II were favorable for OS, and for PFS grade II remained favorable.
Conclusions: In a multicenter collaboration, this trial accrued the highest number of patients published so far, and results are comparable to the best single-institution series. The RT boost, when feasible, seemed effective in improving prognosis. Even after multiple procedures, complete resection confirmed its prognostic strength, along with tumor grade. Biological parameters emerging in this series will be the object of future correlatives and reports.
Keywords: boost; ependymoma; grade; prognosis; surgery.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Pietsch T, Wohlers I, Goschzik T et al. . Supratentorial ependymomas of childhood carry C11orf95-RELA fusions leading to pathological activation of the NF-κB signaling pathway. Acta Neuropathol. 2014;127 (4):609–611. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
