

Racial and Socioeconomic Disparities in Hip Fracture Care
- PMID: 27194496
- PMCID: PMC4866580
- DOI: 10.2106/JBJS.15.00676
Racial and Socioeconomic Disparities in Hip Fracture Care
Abstract
Background: Despite declines in both the incidence of and mortality following hip fracture, there are racial and socioeconomic disparities in treatment access and outcomes. We evaluated the presence and implications of disparities in delivery of care, hypothesizing that race and community socioeconomic characteristics would influence quality of care for patients with a hip fracture.
Methods: We collected data from the New York State Department of Health Statewide Planning and Research Cooperative System (SPARCS), which prospectively captures information on all discharges from nonfederal acute-care hospitals in New York State. Records for 197,290 New York State residents who underwent surgery for a hip fracture between 1998 and 2010 in New York State were identified from SPARCS using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. Multivariable regression models were used to evaluate the association of patient characteristics, social deprivation, and hospital/surgeon volume with time from admission to surgery, in-hospital complications, readmission, and 1-year mortality.
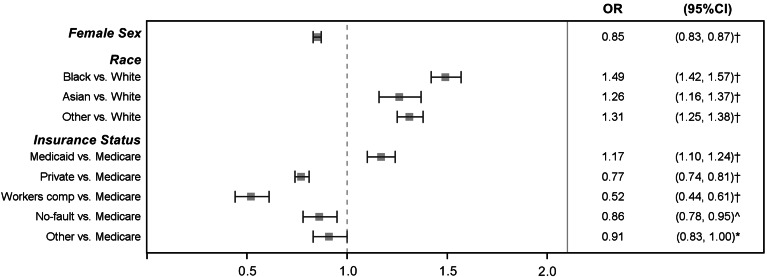
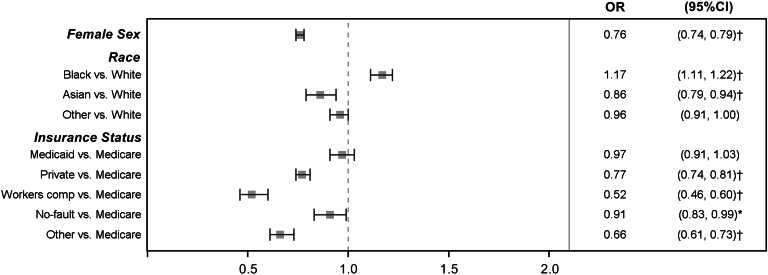
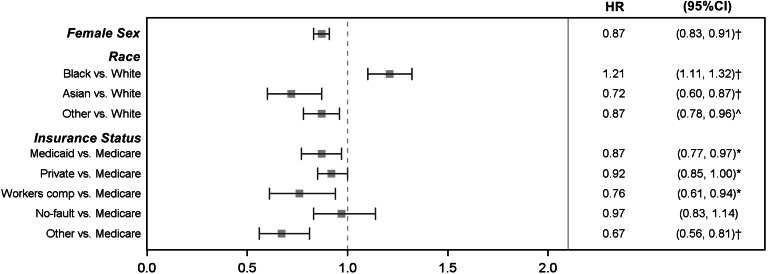
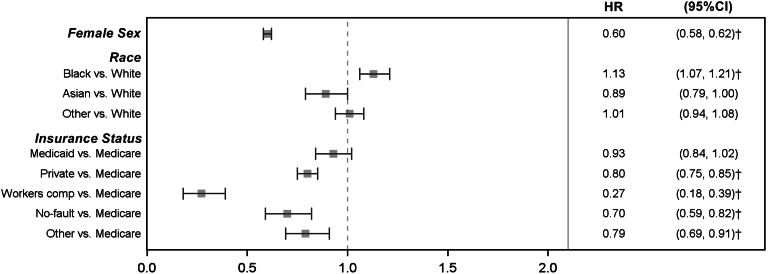
Results: After adjusting for patient and surgery characteristics, hospital/surgeon volume, social deprivation, and other variables, black patients were at greater risk for delayed surgery (odds ratio [OR] = 1.49; 95% confidence interval [CI] = 1.42, 1.57), a reoperation (hazard ratio [HR] = 1.21; CI = 1.11, 1.32), readmission (OR = 1.17; CI = 1.11, 1.22), and 1-year mortality (HR = 1.13; CI = 1.07, 1.21) than white patients. Subgroup analyses showed a greater risk for delayed surgery for black and Asian patients compared with white patients, regardless of social deprivation. Additionally, there was a greater risk for readmission for black patients compared with white patients, regardless of social deprivation. Compared with Medicare patients, Medicaid patients were at increased risk for delayed surgery (OR = 1.17; CI = 1.10, 1.24) whereas privately insured patients were at decreased risk for delayed surgery (OR = 0.77; CI = 0.74, 0.81), readmission (OR = 0.77; CI = 0.74, 0.81), complications (OR = 0.80; CI = 0.77, 0.84), and 1-year mortality (HR = 0.80; CI = 0.75, 0.85).
Conclusions: There are race and insurance-based disparities in delivery of care for patients with hip fracture, some of which persist after adjusting for social deprivation. In addition to investigation into reasons contributing to disparities, targeted interventions should be developed to mitigate effects of disparities on patients at greatest risk.
Level of evidence: Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2016 by The Journal of Bone and Joint Surgery, Incorporated.
Figures
References
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007. March;22(3):465-75. - PubMed
-
- Becker DJ, Arora T, Kilgore ML, Curtis JR, Delzell E, Saag KG, Yun H, Morrisey MA. Trends in the utilization and outcomes of Medicare patients hospitalized for hip fracture, 2000-2008. J Aging Health. 2014. April;26(3):360-79. Epub 2014 Jan 8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
