

Endoscopic endonasal approach to the craniocervical junction: the importance of anterior C1 arch preservation or its reconstruction
- PMID: 27196075
- PMCID: PMC4907157
- DOI: 10.14639/0392-100X-647
Endoscopic endonasal approach to the craniocervical junction: the importance of anterior C1 arch preservation or its reconstruction
Abstract
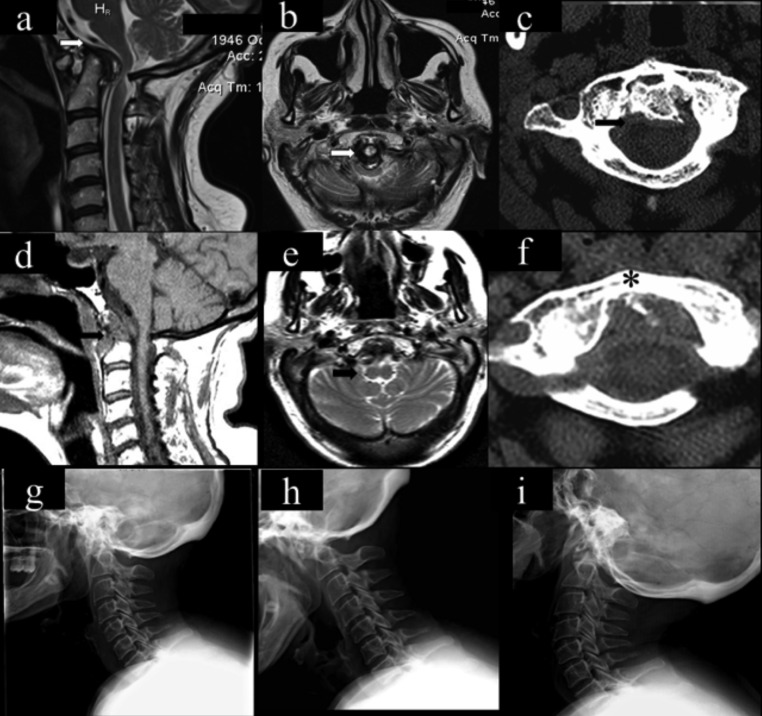
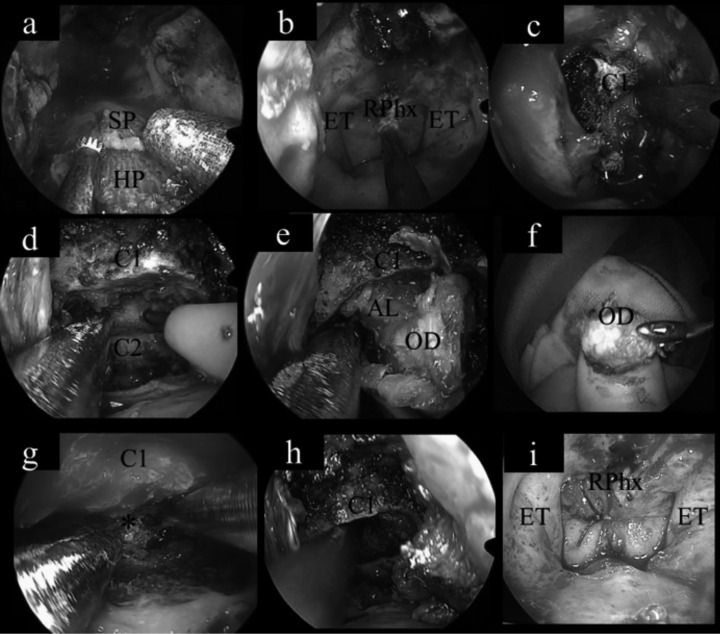
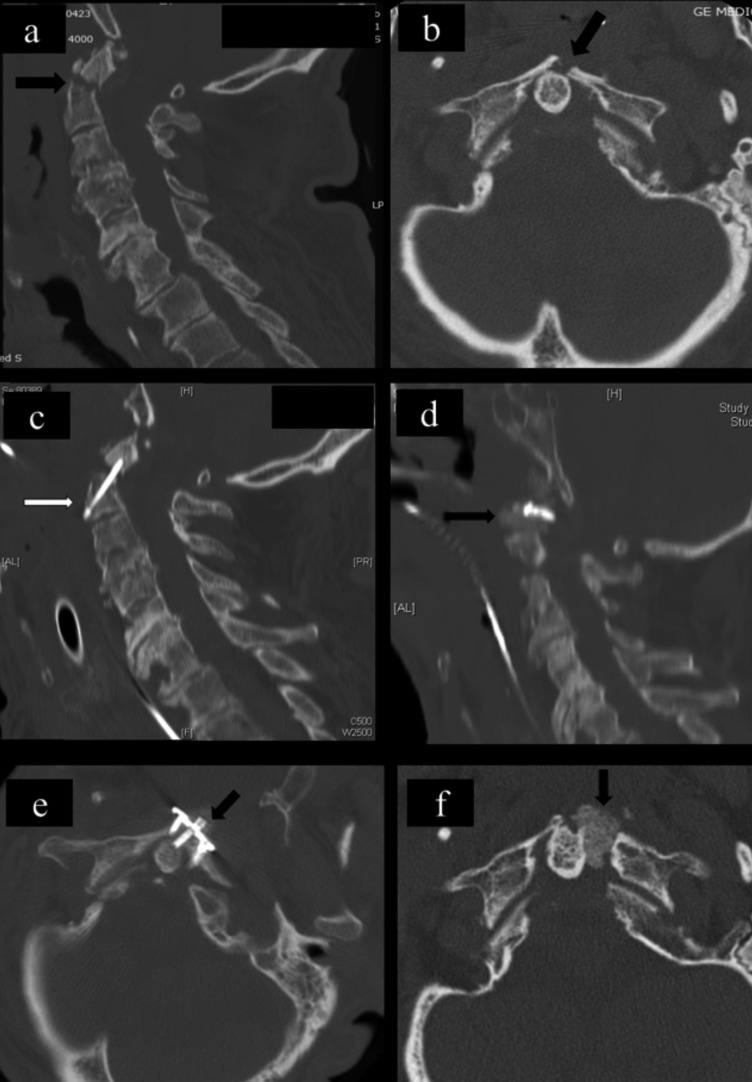
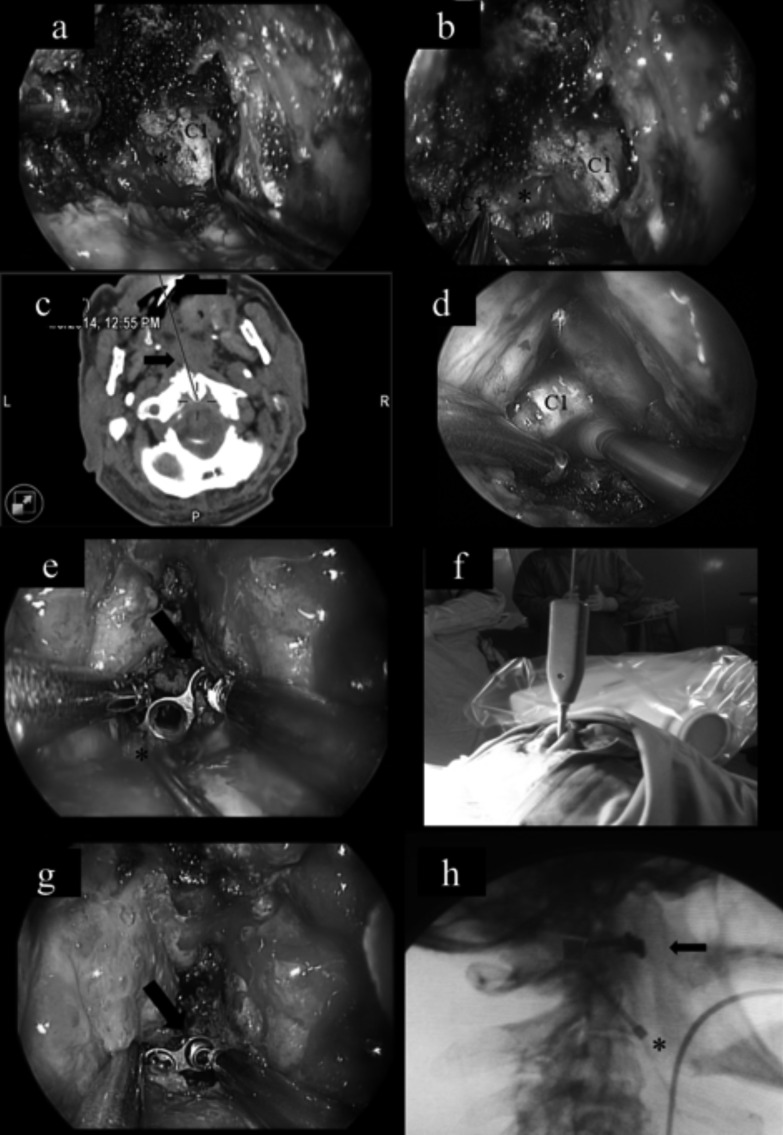
We report our experience with the endoscopic endonasal approaches (EEA) for different craniocervical junction (CCJ) disorders to analyse outcomes and demonstrate the importance and feasibility of anterior C1 arch preservation or its reconstruction. Between January 2009 and December 2013, 10 patients underwent an endoscopic endonasal approach for different CCJ pathologies at our Institution. In 8 patients we were able to preserve the anterior C1 arch, while in 2 post-traumatic cases we reconstructed it. The CCJ disorders included 4 cases of irreducible anterior bulbo-medullary compression secondary to rheumatoid arthritis or CCJ anomalies, 4 cases of inveterate fractures of C1 and/or C2 and 2 tumours. Pre- and postoperative neuroradiological evaluation was always obtained by magnetic resonance imaging (MRI), computed tomographic (CT) scanning and dynamic cranio-vertebral junction x-ray. Pre- and postoperative neurologic disability assessment was obtained by Ranawat classification for patients with rheumatoid arthritis and by Nurick classification for the others. At a mean follow-up of 31 months (range: 14-73 months), an improvement of at least one Ranawat or Nurick classification level was observed in 6 patients, while in another 4 patients neurological conditions were stable. Radiological follow-up revealed an adequate bulbo-medullary decompression in all patients and a regular bone fusion in cases of C1 and/or C2 fractures. In all patients spinal stability was preserved and none required subsequent posterior fixation. The endoscopic endonasal surgery provided adequate exposure and a low morbidity minimally invasive approach to the antero-medial located lesions of the CCJ, resulting in a safe, effective and well-tolerated procedure. This approach allowed preservation of the anterior C1 arch and the avoidance of a posterior fixation in all patients of this series, thus preserving the rotational movement at C0-C2 segment and reducing the risk of a subaxial instability development.
Riportiamo la nostra esperienza con l’approccio endoscopico endonasale (EEA) in una serie consecutiva di 10 pazienti affetti da lesioni anteriori della giunzione cranio-cervicale. L’obiettivo dello studio è analizzare l’outcome di questi pazienti focalizzando l’attenzione sulla possibilità di preservare o ricostruire l’arco anteriore di C1, quale importante elemento di stabilità della giunzione cranio-cervicale. Dal gennaio 2009 al dicembre 2013, 10 pazienti con patologia della giunzione craniocervicale sono stati operati mediante approccio endoscopico endonasale. Le lesioni trattate includevano 4 casi di non riducibile compressione bulbo-midollare extradurale anteriore della giunzione (secondarie ad artrite reumatoide o anomalie della giunzione), 4 casi di fratture inveterate di C1 o del dente dell’epistrofeo e 2 casi lesioni tumorali. La valutazione clinica pre- e postoperatoria è stata effettuata mediante la scala di Ranawat per i casi di artrite reumatoide e di Nurick per gli altri. Il follow-up radiologico comprendeva invece RM, TC e RX con prove morfo-dinamiche per eventuale preesistente severa instabilità. Dopo l’approccio EEA puro alla giunzione craniocervicale, nessun paziente ha presentato un peggioramento neurologico, né si sono verificate significative complicanze. Al follow-up medio di 31 mesi (range 14-73 mesi), un miglioramento di almeno un livello della classificazione Ranawat o Nurick si è osservato in 6 pazienti mentre gli altri 4 sono rimasti stabili. Il follow-up neuroradiologico ha documentato in tutti i casi un’adeguata decompressione bulbo-midollare, mentre nei casi di frattura di C1 o C2 una regolare fusione ossea delle rime di frattura. Nessun paziente ha presentato segni di instabilità e non è stata pertanto necessaria alcuna procedura di stabilizzazione e fusione posteriore. L’approccio endoscopico endonasale garantisce un’adeguata esposizione delle lesioni antero-mediali della giunzione craniocervicale. Nella nostra serie di pazienti tale procedura ha permesso di preservare o ricostruire l’arco anteriore di C1, evitando quindi una sintesi posteriore e la relativa perdita di movimento rotazionale C0-C2 e l’instabilità subassiale.
Keywords: Anterior C1 arch preservation; C2 odontoidectomy; Endoscopic endonasal surgery; Spine instability.
© Copyright by Società Italiana di Otorinolaringologia e Chirurgia Cervico-Facciale, Rome, Italy.
Figures
Comment in
-
Considerations on "Endoscopic endonasal approach to the craniocervical junction: the importance of anterior C1 arch preservation or its reconstruction".Acta Otorhinolaryngol Ital. 2016 Jun;36(3):228-30. doi: 10.14639/0392-100X-927. Acta Otorhinolaryngol Ital. 2016. PMID: 27214835 Free PMC article. No abstract available.
Similar articles
-
Endoscopic endonasal odontoidectomy with anterior C1 arch preservation in elderly patients affected by rheumatoid arthritis.Spine J. 2013 May;13(5):542-8. doi: 10.1016/j.spinee.2013.01.043. Epub 2013 Mar 1. Spine J. 2013. PMID: 23453575
-
Endoscopic Endonasal Odontoidectomy with Anterior C1 Arch Preservation in Rheumatoid Arthritis: Long-Term Follow-Up and Further Technical Improvement by Anterior Endoscopic C1-C2 Screw Fixation and Fusion.World Neurosurg. 2017 Nov;107:820-829. doi: 10.1016/j.wneu.2017.08.063. Epub 2017 Aug 24. World Neurosurg. 2017. PMID: 28842239
-
Advantages and limitations of endoscopic endonasal odontoidectomy. A series of nine cases.Orthop Traumatol Surg Res. 2014 Nov;100(7):775-8. doi: 10.1016/j.otsr.2014.07.017. Epub 2014 Oct 1. Orthop Traumatol Surg Res. 2014. PMID: 25281548
-
Basilar Invagination: Case Report and Literature Review.World Neurosurg. 2015 Jun;83(6):1180.e7-11. doi: 10.1016/j.wneu.2015.02.007. Epub 2015 Feb 18. World Neurosurg. 2015. PMID: 25701769 Review.
-
Odontoid-sparing transnasal approach for drainage of craniocervical epidural abscess; a novel technique and review of the literature.Spine J. 2018 Mar;18(3):540-546. doi: 10.1016/j.spinee.2017.12.008. Epub 2017 Dec 15. Spine J. 2018. PMID: 29253634 Review.
Cited by
-
Coil Extrusion into the Naso- and Oropharynx Ten Years after Internal Carotid Artery Pseudoaneurysm Embolization: A Case Report.Case Rep Neurol. 2019 Jan 17;11(1):4-9. doi: 10.1159/000496283. eCollection 2019 Jan-Apr. Case Rep Neurol. 2019. PMID: 30792650 Free PMC article.
-
Sixth Cranial Nerve Palsy and Craniocervical Junction Instability due to Metastatic Urothelial Bladder Carcinoma.Case Rep Neurol. 2019 Jan 30;11(1):24-31. doi: 10.1159/000496419. eCollection 2019 Jan-Apr. Case Rep Neurol. 2019. PMID: 31543783 Free PMC article.
-
Endoscopic transnasal skull base surgery: pushing the boundaries.J Neurooncol. 2016 Nov;130(2):319-330. doi: 10.1007/s11060-016-2274-y. Epub 2016 Oct 20. J Neurooncol. 2016. PMID: 27766473 Review.
-
Endoscopic endonasal odontoidectomy: a long-term follow-up results for a cohort of 21 patients.Eur Spine J. 2022 Oct;31(10):2693-2703. doi: 10.1007/s00586-022-07308-6. Epub 2022 Jul 20. Eur Spine J. 2022. PMID: 35859067
-
Evolution of Cervical Endoscopic Spine Surgery: Current Progress and Future Directions-A Narrative Review.J Clin Med. 2024 Apr 6;13(7):2122. doi: 10.3390/jcm13072122. J Clin Med. 2024. PMID: 38610887 Free PMC article. Review.
References
-
- Blazier CJ, Hadley MN, Spetzler RF. The transoral surgical approach to craniovertebral pathology. J Neurosci Nurs. 1986;18:57–62. - PubMed
-
- Baird CJ, Conway JE, Sciubba DM, et al. Radiographic and anatomic basis of endoscopic anterior craniocervical decompression: a comparison of endonasal, transoral, and transcervical approaches. Neurosurgery. 2009;65(Suppl 6):158–163. - PubMed
-
- Kassam AB, Snyderman C, Gaedner P, et al. The expanded endonasal approach: a fully endoscopic endonasal approach and resection of the odontoid process: technical case report. Neurosurgery. 2005;57(Suppl 1):E213–E213. - PubMed
-
- Alfieri A, Jho HD, Tschabitscher M. Endoscopic endonasal approach to the ventral craniocervical junction: anatomical study. Acta Neurochir. 2002;144:219–225. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
