

Predicting Mortality in Low-Income Country ICUs: The Rwanda Mortality Probability Model (R-MPM)
- PMID: 27196252
- PMCID: PMC4873171
- DOI: 10.1371/journal.pone.0155858
Predicting Mortality in Low-Income Country ICUs: The Rwanda Mortality Probability Model (R-MPM)
Abstract
Introduction: Intensive Care Unit (ICU) risk prediction models are used to compare outcomes for quality improvement initiatives, benchmarking, and research. While such models provide robust tools in high-income countries, an ICU risk prediction model has not been validated in a low-income country where ICU population characteristics are different from those in high-income countries, and where laboratory-based patient data are often unavailable. We sought to validate the Mortality Probability Admission Model, version III (MPM0-III) in two public ICUs in Rwanda and to develop a new Rwanda Mortality Probability Model (R-MPM) for use in low-income countries.
Methods: We prospectively collected data on all adult patients admitted to Rwanda's two public ICUs between August 19, 2013 and October 6, 2014. We described demographic and presenting characteristics and outcomes. We assessed the discrimination and calibration of the MPM0-III model. Using stepwise selection, we developed a new logistic model for risk prediction, the R-MPM, and used bootstrapping techniques to test for optimism in the model.
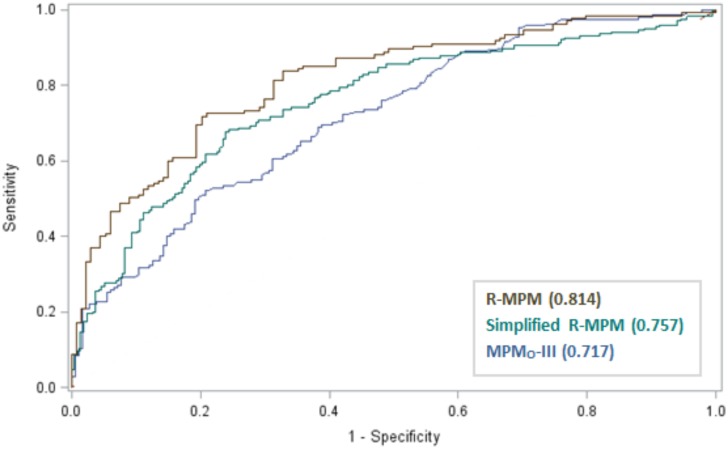
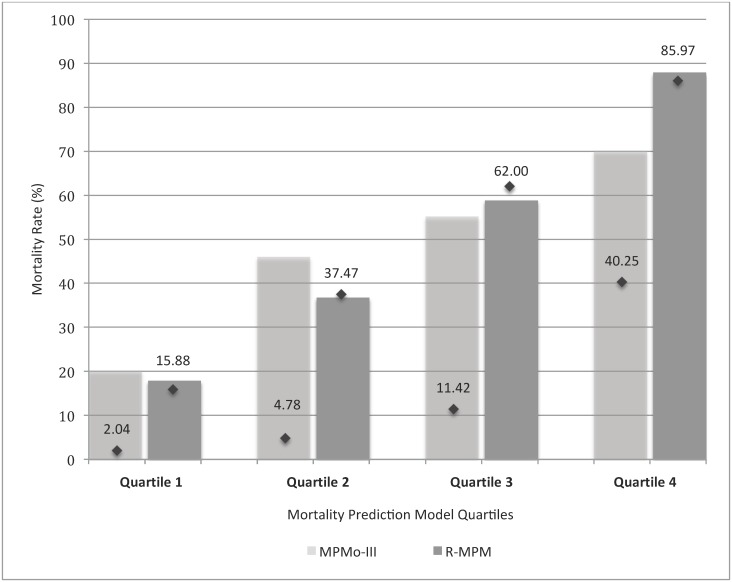
Results: Among 427 consecutive adults, the median age was 34 (IQR 25-47) years and mortality was 48.7%. Mechanical ventilation was initiated for 85.3%, and 41.9% received vasopressors. The MPM0-III predicted mortality with area under the receiver operating characteristic curve of 0.72 and Hosmer-Lemeshow chi-square statistic p = 0.024. We developed a new model using five variables: age, suspected or confirmed infection within 24 hours of ICU admission, hypotension or shock as a reason for ICU admission, Glasgow Coma Scale score at ICU admission, and heart rate at ICU admission. Using these five variables, the R-MPM predicted outcomes with area under the ROC curve of 0.81 with 95% confidence interval of (0.77, 0.86), and Hosmer-Lemeshow chi-square statistic p = 0.154.
Conclusions: The MPM0-III has modest ability to predict mortality in a population of Rwandan ICU patients. The R-MPM is an alternative risk prediction model with fewer variables and better predictive power. If validated in other critically ill patients in a broad range of settings, the model has the potential to improve the reliability of comparisons used for critical care research and quality improvement initiatives in low-income countries.
Conflict of interest statement
Figures
References
-
- Keegan MT, Gajic O, Afessa B. Severity of illness scoring systems in the intensive care unit. Crit Care Med. 2011;39(1):163–9. Epub 2010/09/15. . - PubMed
-
- Knaus WA, Zimmerman JE, Wagner DP, Draper EA, Lawrence DE. APACHE-acute physiology and chronic health evaluation: a physiologically based classification system. Crit Care Med. 1981;9(8):591–7. Epub 1981/08/01. . - PubMed
-
- Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of Acute Physiology And Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41(7):1711–8. Epub 2013/05/11. . - PubMed
-
- Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients. Crit Care Med. 2006;34(5):1297–310. Epub 2006/03/17. . - PubMed
-
- Higgins TL, Kramer AA, Nathanson BH, Copes W, Stark M, Teres D. Prospective validation of the intensive care unit admission Mortality Probability Model (MPM0-III). Crit Care Med. 2009;37(5):1619–23. Epub 2009/03/28. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
