

Narrow band imaging optical diagnosis of small colorectal polyps in routine clinical practice: the Detect Inspect Characterise Resect and Discard 2 (DISCARD 2) study
- PMID: 27196576
- PMCID: PMC5531217
- DOI: 10.1136/gutjnl-2015-310584
Narrow band imaging optical diagnosis of small colorectal polyps in routine clinical practice: the Detect Inspect Characterise Resect and Discard 2 (DISCARD 2) study
Abstract
Background: Accurate optical characterisation and removal of small adenomas (<10 mm) at colonoscopy would allow hyperplastic polyps to be left in situ and surveillance intervals to be determined without the need for histopathology. Although accurate in specialist practice the performance of narrow band imaging (NBI), colonoscopy in routine clinical practice is poorly understood.
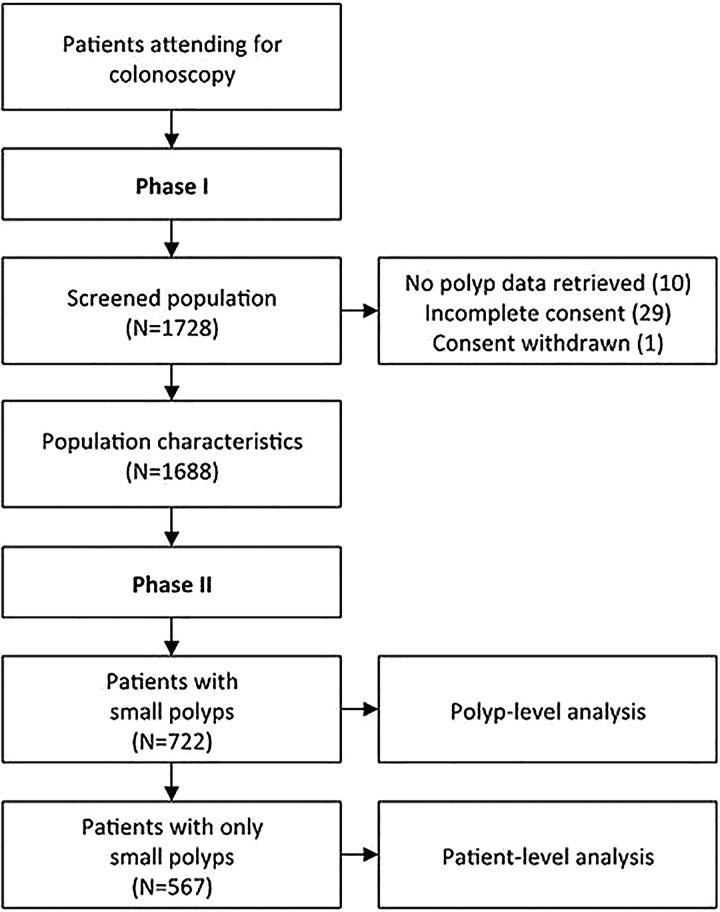
Methods: NBI-assisted optical diagnosis was compared with reference standard histopathological findings in a prospective, blinded study, which recruited adults undergoing routine colonoscopy in six general hospitals in the UK. Participating colonoscopists (N=28) were trained using the NBI International Colorectal Endoscopic (NICE) classification (relating to colour, vessel structure and surface pattern). By comparing the optical and histological findings in patients with only small polyps, test sensitivity was determined at the patient level using two thresholds: presence of adenoma and need for surveillance. Accuracy of identifying adenomatous polyps <10 mm was compared at the polyp level using hierarchical models, allowing determinants of accuracy to be explored.
Findings: Of 1688 patients recruited, 722 (42.8%) had polyps <10 mm with 567 (78.5%) having only polyps <10 mm. Test sensitivity (presence of adenoma, N=499 patients) by NBI optical diagnosis was 83.4% (95% CI 79.6% to 86.9%), significantly less than the 95% sensitivity (p<0.001) this study was powered to detect. Test sensitivity (need for surveillance) was 73.0% (95% CI 66.5% to 79.9%). Analysed at the polyp level, test sensitivity (presence of adenoma, N=1620 polyps) was 76.1% (95% CI 72.8% to 79.1%). In fully adjusted analyses, test sensitivity was 99.4% (95% CI 98.2% to 99.8%) if two or more NICE adenoma characteristics were identified. Neither colonoscopist expertise, confidence in diagnosis nor use of high definition colonoscopy independently improved test accuracy.
Interpretation: This large multicentre study demonstrates that NBI optical diagnosis cannot currently be recommended for application in routine clinical practice. Further work is required to evaluate whether variation in test accuracy is related to polyp characteristics or colonoscopist training.
Trial registration number: The study was registered with clinicaltrials.gov (NCT01603927).
Keywords: COLONIC NEOPLASMS; COLONOSCOPY; COLORECTAL ADENOMAS; ENDOSCOPY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Comment in
-
New-generation chromoendoscopy may increase confidence in the DISCARD2 study.Gut. 2018 Sep;67(9):1742-1743. doi: 10.1136/gutjnl-2017-314999. Epub 2017 Oct 11. Gut. 2018. PMID: 29021210 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical