

A Tissue Systems Pathology Assay for High-Risk Barrett's Esophagus
- PMID: 27197290
- PMCID: PMC4891291
- DOI: 10.1158/1055-9965.EPI-15-1164
A Tissue Systems Pathology Assay for High-Risk Barrett's Esophagus
Abstract
Background: Better methods are needed to predict risk of progression for Barrett's esophagus. We aimed to determine whether a tissue systems pathology approach could predict progression in patients with nondysplastic Barrett's esophagus, indefinite for dysplasia, or low-grade dysplasia.
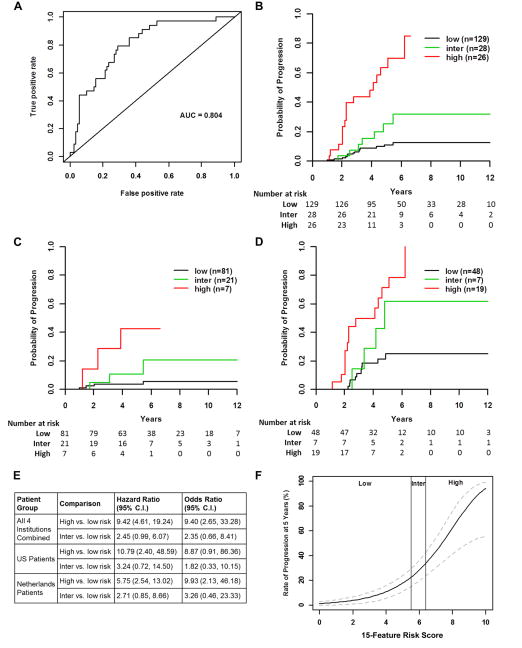
Methods: We performed a nested case-control study to develop and validate a test that predicts progression of Barrett's esophagus to high-grade dysplasia (HGD) or esophageal adenocarcinoma (EAC), based upon quantification of epithelial and stromal variables in baseline biopsies. Data were collected from Barrett's esophagus patients at four institutions. Patients who progressed to HGD or EAC in ≥1 year (n = 79) were matched with patients who did not progress (n = 287). Biopsies were assigned randomly to training or validation sets. Immunofluorescence analyses were performed for 14 biomarkers and quantitative biomarker and morphometric features were analyzed. Prognostic features were selected in the training set and combined into classifiers. The top-performing classifier was assessed in the validation set.
Results: A 3-tier, 15-feature classifier was selected in the training set and tested in the validation set. The classifier stratified patients into low-, intermediate-, and high-risk classes [HR, 9.42; 95% confidence interval, 4.6-19.24 (high-risk vs. low-risk); P < 0.0001]. It also provided independent prognostic information that outperformed predictions based on pathology analysis, segment length, age, sex, or p53 overexpression.
Conclusion: We developed a tissue systems pathology test that better predicts risk of progression in Barrett's esophagus than clinicopathologic variables.
Impact: The test has the potential to improve upon histologic analysis as an objective method to risk stratify Barrett's esophagus patients. Cancer Epidemiol Biomarkers Prev; 25(6); 958-68. ©2016 AACR.
©2016 American Association for Cancer Research.
Figures


References
-
- Wani S, Falk G, Hall M, Gaddam S, Wang A, Gupta N, et al. Patients with nondysplastic Barrett's esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol. 2011;9:220–7. quiz e26. - PubMed
-
- Wani S, Falk GW, Post J, Yerian L, Hall M, Wang A, et al. Risk factors for progression of low-grade dysplasia in patients with Barrett's esophagus. Gastroenterology. 2011;141:1179–86. 1186 e1. - PubMed
-
- Thota PN, Lee HJ, Goldblum JR, Liu X, Sanaka MR, Gohel T, et al. Risk stratification of patients with barrett's esophagus and low-grade dysplasia or indefinite for dysplasia. Clin Gastroenterol Hepatol. 2014;13:459–465 e1. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
