

Impact of Ejection Fraction and Aortic Valve Gradient on Outcomes of Transcatheter Aortic Valve Replacement
- PMID: 27199058
- PMCID: PMC5372353
- DOI: 10.1016/j.jacc.2016.03.514
Impact of Ejection Fraction and Aortic Valve Gradient on Outcomes of Transcatheter Aortic Valve Replacement
Abstract
Background: In patients with aortic stenosis undergoing transcatheter aortic valve replacement (TAVR), studies have suggested that reduced left ventricular (LV) ejection fraction (LVEF) and low aortic valve gradient (AVG) are associated with worse long-term outcomes. Because these conditions commonly coexist, the extent to which they are independently associated with outcomes after TAVR is unknown.
Objectives: The purpose of this study was to evaluate the impact of LVEF and AVG on clinical outcomes after TAVR and to determine whether the effect of AVG on outcomes is modified by LVEF.
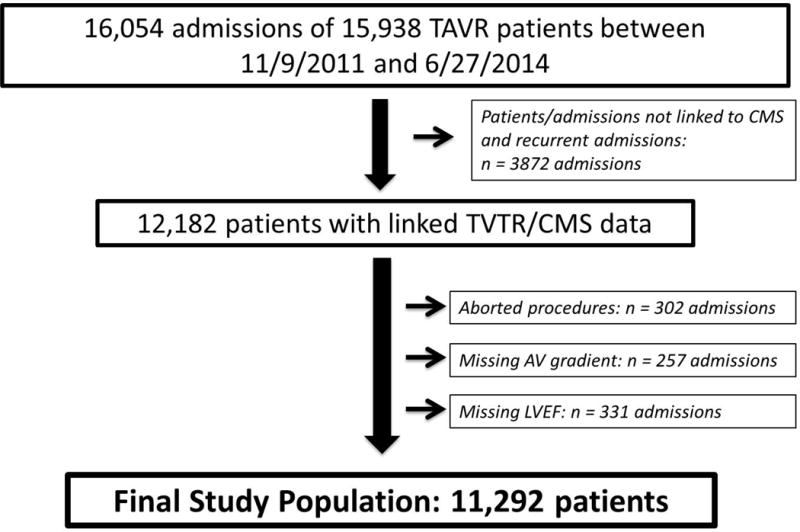
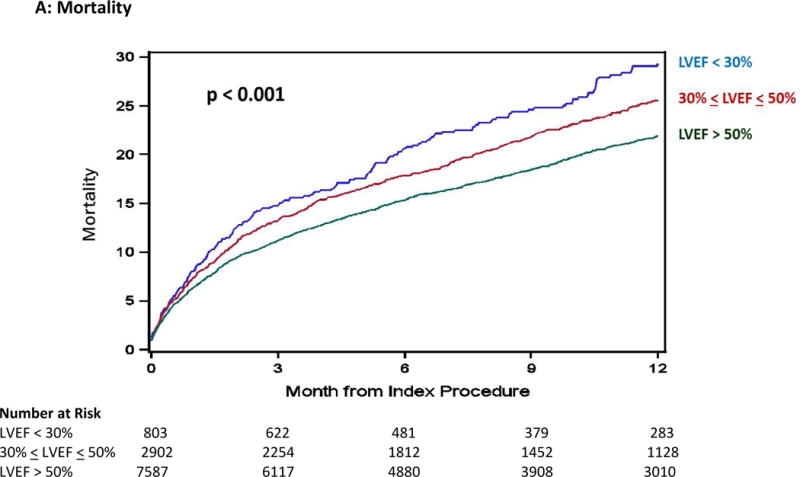
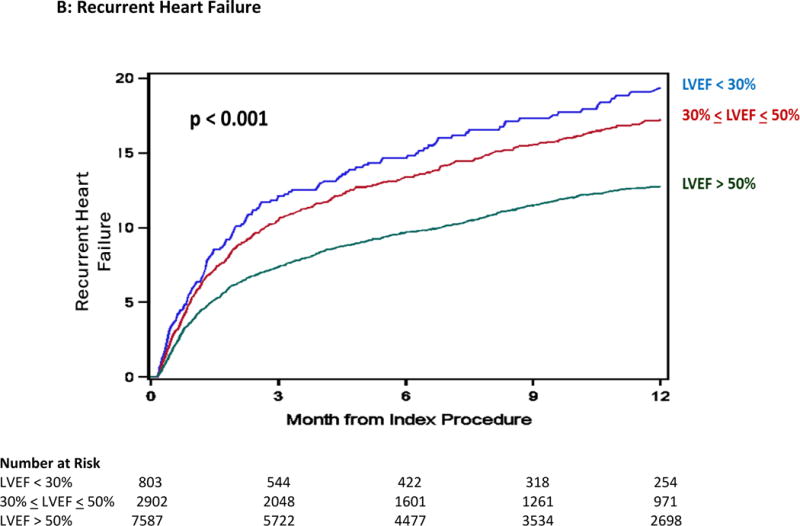
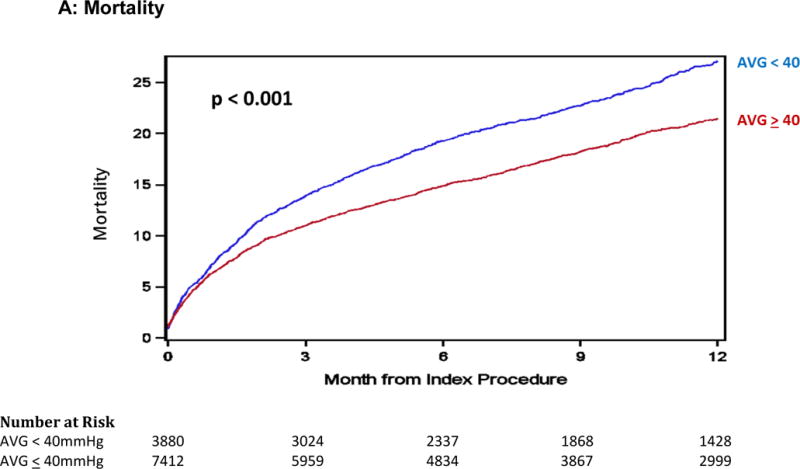
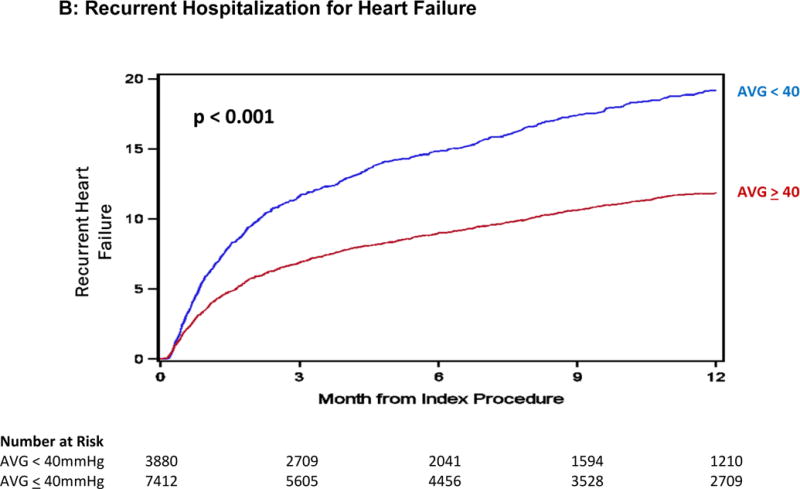
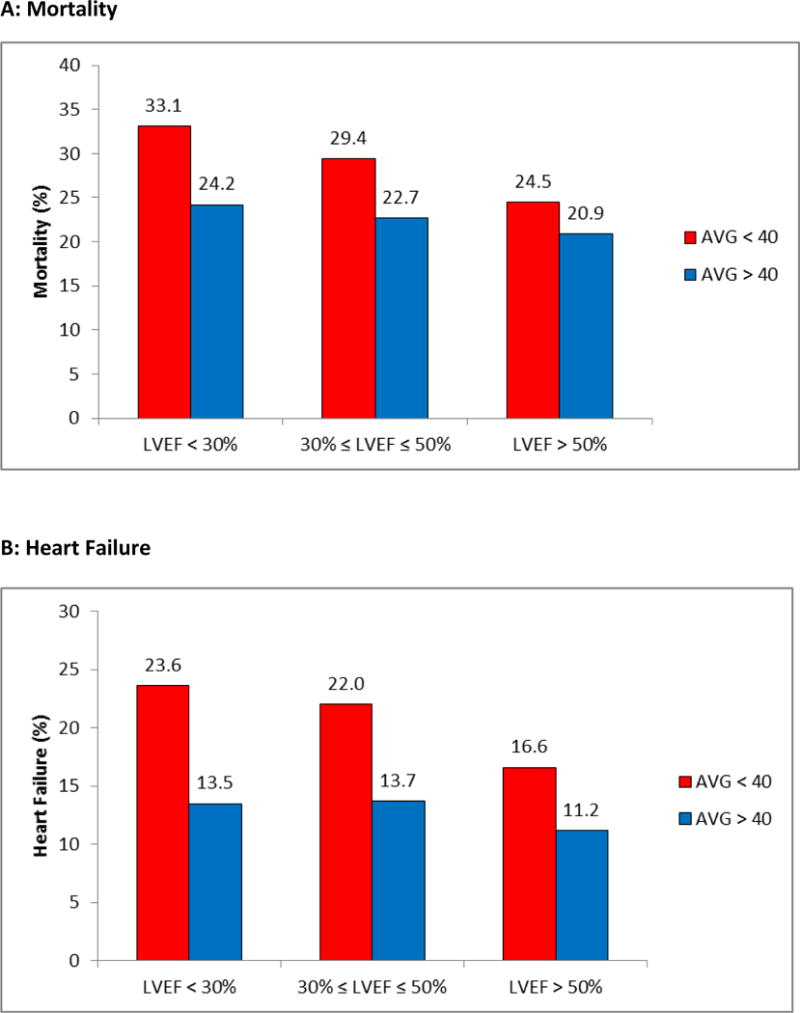
Methods: Using data from 11,292 patients who underwent TAVR as part of the Transcatheter Valve Therapies Registry, we examined rates of 1-year mortality and recurrent heart failure in patients with varying levels of LV dysfunction (LVEF <30% vs. 30% to 50% vs. >50%) and AVG (<40 mm Hg vs. ≥40 mm Hg). Multivariable models were used to estimate the independent effect of AVG and LVEF on outcomes.
Results: During the first year of follow-up after TAVR, patients with LV dysfunction and low AVG had higher rates of death and recurrent heart failure. After adjustment for other clinical factors, only low AVG was associated with higher mortality (hazard ratio: 1.21; 95% confidence interval: 1.11 to 1.32; p < 0.001) and higher rates of heart failure (hazard ratio: 1.52; 95% confidence interval: 1.36 to 1.69; p <0.001), whereas the effect of LVEF was no longer significant. There was no evidence of effect modification between AVG and LVEF with respect to either endpoint.
Conclusions: In this series of real-world patients undergoing TAVR, low AVG, but not LV dysfunction, was associated with higher rates of mortality and recurrent heart failure. Although these findings suggest that AVG should be considered when evaluating the risks and benefits of TAVR for individual patients, neither severe LV dysfunction nor low AVG alone or in combination provide sufficient prognostic discrimination to preclude treatment with TAVR.
Keywords: AV gradient; LVEF; TAVR; left ventricular dysfunction; stroke; surgical aortic valve replacement.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
The Complex Interaction Between Left Ventricular Ejection Fraction, Flow, and Gradient in Patients Undergoing TAVR.J Am Coll Cardiol. 2016 May 24;67(20):2359-2363. doi: 10.1016/j.jacc.2016.02.072. J Am Coll Cardiol. 2016. PMID: 27199059 No abstract available.
Similar articles
-
Outcomes of transcatheter and surgical aortic valve replacement in high-risk patients with aortic stenosis and left ventricular dysfunction: results from the Placement of Aortic Transcatheter Valves (PARTNER) trial (cohort A).Circ Cardiovasc Interv. 2013 Dec;6(6):604-14. doi: 10.1161/CIRCINTERVENTIONS.113.000650. Epub 2013 Nov 12. Circ Cardiovasc Interv. 2013. PMID: 24221391 Clinical Trial.
-
Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis: The TOPAS-TAVI Registry.J Am Coll Cardiol. 2018 Mar 27;71(12):1297-1308. doi: 10.1016/j.jacc.2018.01.054. J Am Coll Cardiol. 2018. PMID: 29566812
-
Impact of flow, gradient, and left ventricular function on outcomes after transcatheter aortic valve replacement.Catheter Cardiovasc Interv. 2018 Mar 1;91(4):798-805. doi: 10.1002/ccd.27347. Epub 2017 Oct 8. Catheter Cardiovasc Interv. 2018. PMID: 28988432 Free PMC article.
-
Prognostic Value of Preprocedural LV Global Longitudinal Strain for Post-TAVR-Related Morbidity and Mortality: A Meta-Analysis.JACC Cardiovasc Imaging. 2023 Mar;16(3):332-341. doi: 10.1016/j.jcmg.2023.01.005. JACC Cardiovasc Imaging. 2023. PMID: 36889849
-
The role of TAVR in patients with heart failure: do we have the responses to all questions?Heart Fail Rev. 2022 Sep;27(5):1617-1625. doi: 10.1007/s10741-021-10206-6. Epub 2022 Jan 18. Heart Fail Rev. 2022. PMID: 35039999 Review.
Cited by
-
Outcomes after transcatheter aortic valve replacement in patients with low versus high gradient severe aortic stenosis in the setting of preserved left ventricular ejection fraction.J Interv Cardiol. 2018 Dec;31(6):849-860. doi: 10.1111/joic.12561. Epub 2018 Sep 10. J Interv Cardiol. 2018. PMID: 30203608 Free PMC article.
-
Low-flow in aortic valve stenosis patients with reduced ejection fraction does not depend on left ventricular function.Clin Res Cardiol. 2024 Jan 18. doi: 10.1007/s00392-023-02372-4. Online ahead of print. Clin Res Cardiol. 2024. PMID: 38236417
-
Transcatheter and surgical aortic valve replacement in patients with left ventricular dysfunction.J Cardiothorac Surg. 2022 Dec 18;17(1):322. doi: 10.1186/s13019-022-02061-9. J Cardiothorac Surg. 2022. PMID: 36529781 Free PMC article. Clinical Trial.
-
Current issues in transcatheter aortic valve replacement.J Thorac Dis. 2020 Apr;12(4):1665-1680. doi: 10.21037/jtd.2020.01.10. J Thorac Dis. 2020. PMID: 32395310 Free PMC article. Review.
-
Comparative Analysis of the Kinetic Behavior of Systemic Inflammatory Markers in Patients with Depressed versus Preserved Left Ventricular Function Undergoing Transcatheter Aortic Valve Implantation.J Clin Med. 2021 Sep 15;10(18):4148. doi: 10.3390/jcm10184148. J Clin Med. 2021. PMID: 34575259 Free PMC article.
References
-
- Halkos ME, Chen EP, Sarin EL, et al. Aortic valve replacement for aortic stenosis in patients with left ventricular dysfunction. Ann Thorac Surg. 2009;88:746–51. - PubMed
-
- Pai RG, Varadarajan P, Razzouk A. Survival benefit of aortic valve replacement in patients with severe aortic stenosis with low ejection fraction and low gradient with normal ejection fraction. Ann Thorac Surg. 2008;86:1781–9. - PubMed
-
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. - PubMed
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. - PubMed
-
- Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
