

Association of Guideline-Based Admission Treatments and Life Expectancy After Myocardial Infarction in Elderly Medicare Beneficiaries
- PMID: 27199062
- PMCID: PMC5097252
- DOI: 10.1016/j.jacc.2016.03.507
Association of Guideline-Based Admission Treatments and Life Expectancy After Myocardial Infarction in Elderly Medicare Beneficiaries
Abstract
Background: Guideline-based admission therapies for acute myocardial infarction (AMI) significantly improve 30-day survival, but little is known about their association with long-term outcomes.
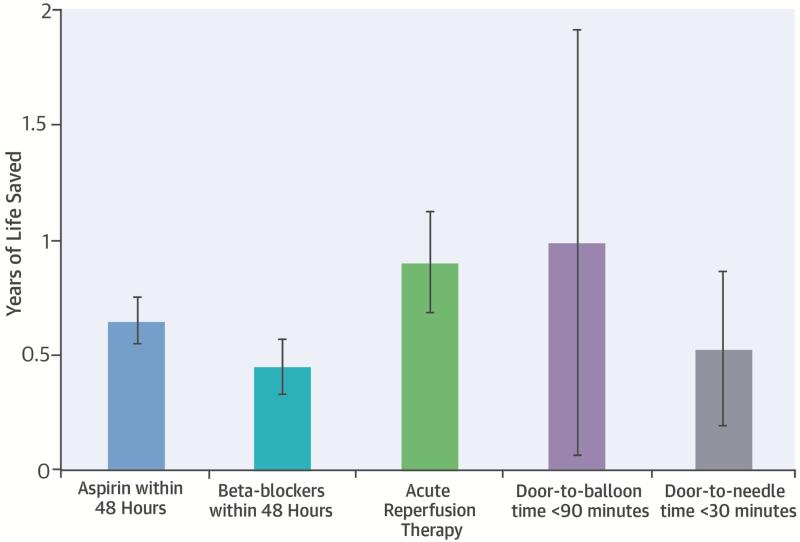
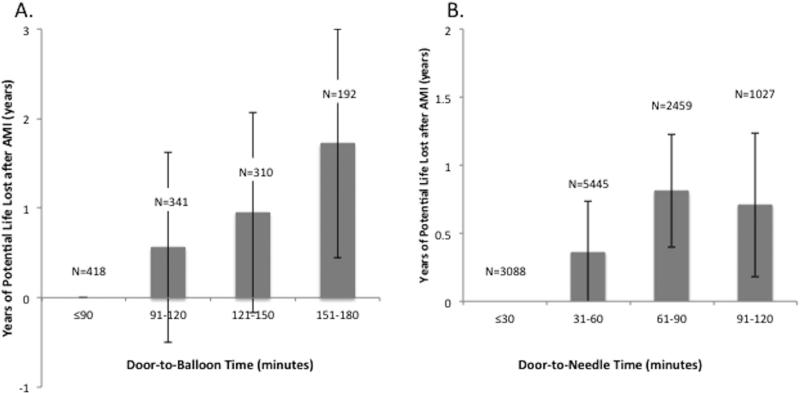
Objectives: This study evaluated the association of 5 AMI admission therapies (aspirin, beta-blockers, acute reperfusion therapy, door-to-balloon [D2B] time ≤90 min, and time to fibrinolysis ≤30 min) with life expectancy and years of life saved after AMI.
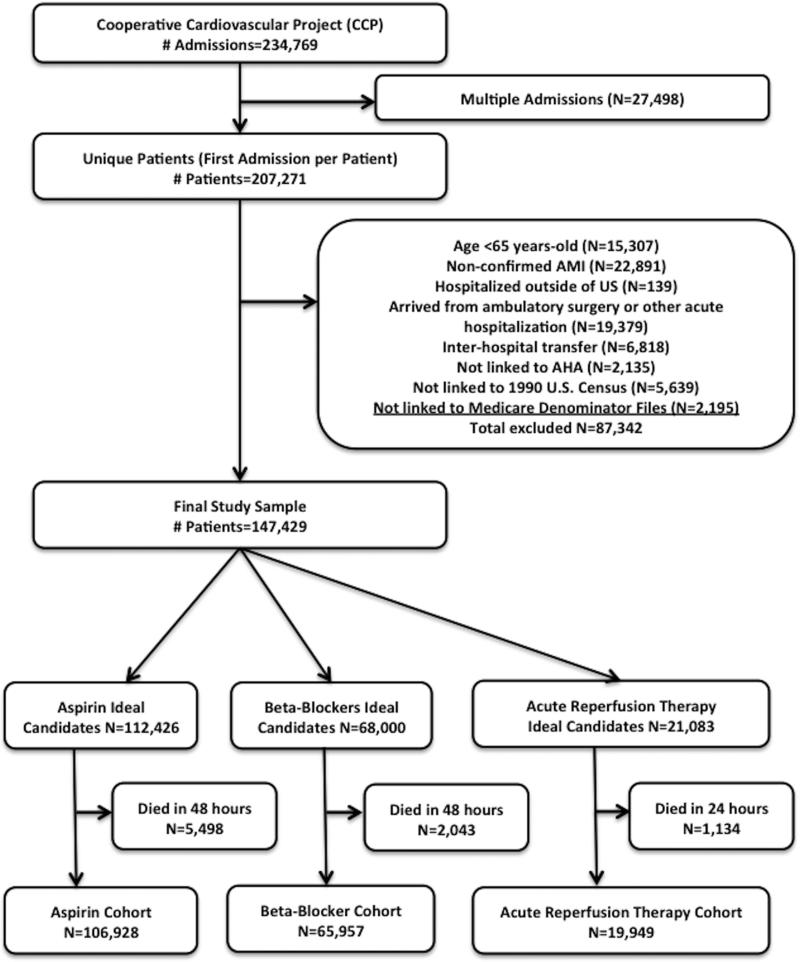
Methods: We analyzed data from the Cooperative Cardiovascular Project, a study of Medicare beneficiaries hospitalized for AMI, with 17 years of follow-up. Life expectancy and years of life saved after AMI were calculated using Cox proportional hazards regression with extrapolation using exponential models.
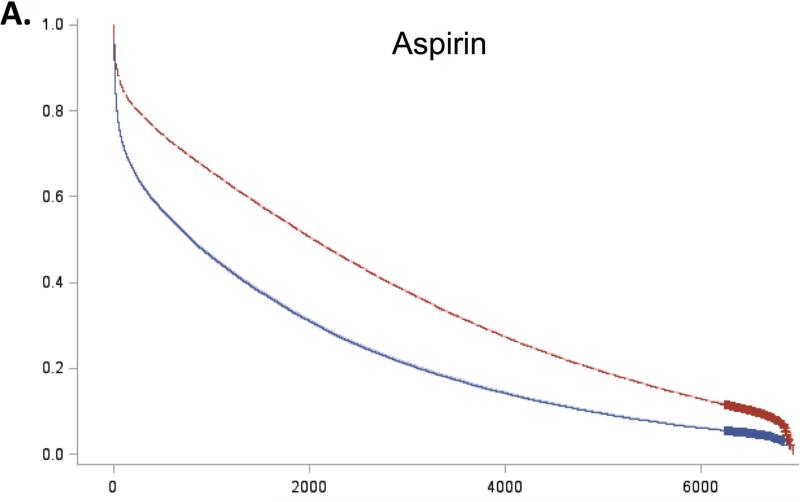
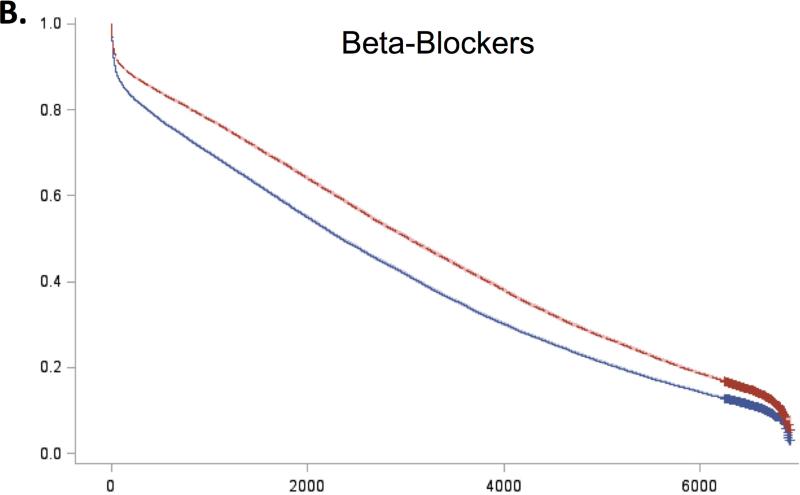
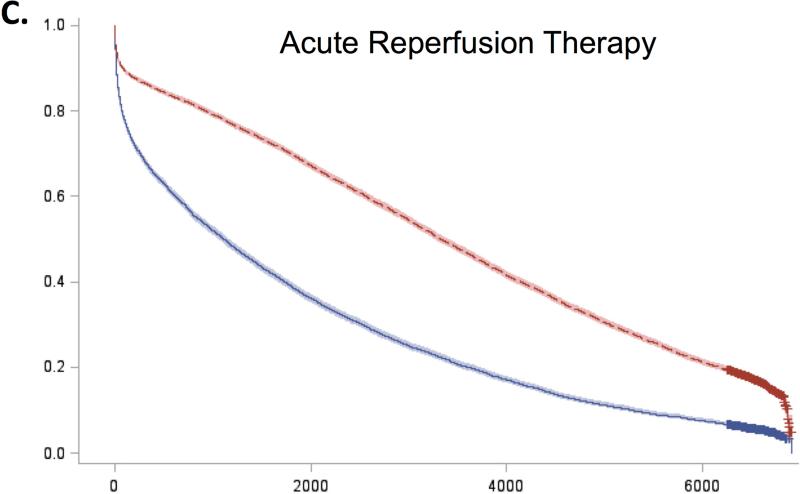
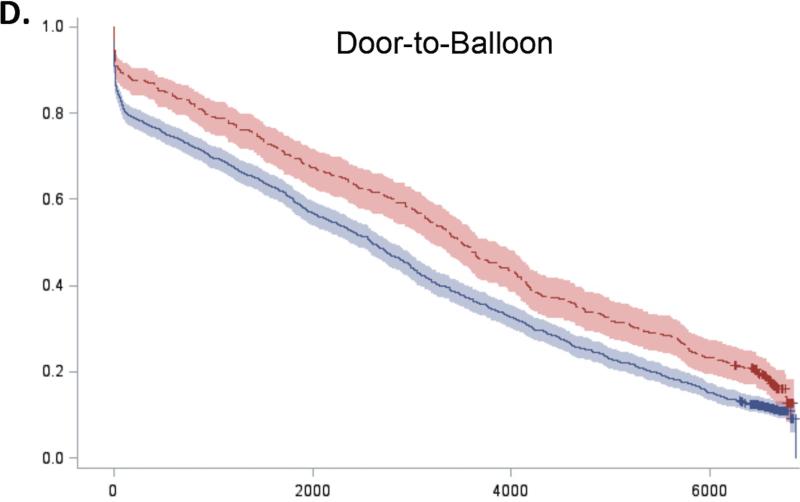
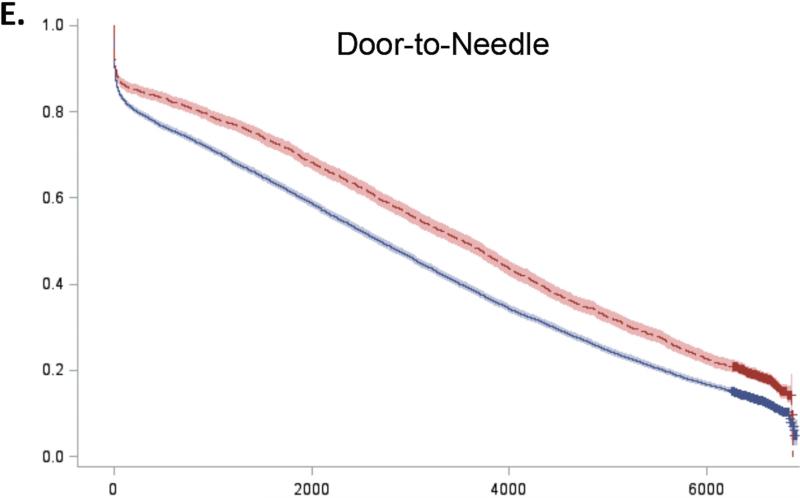
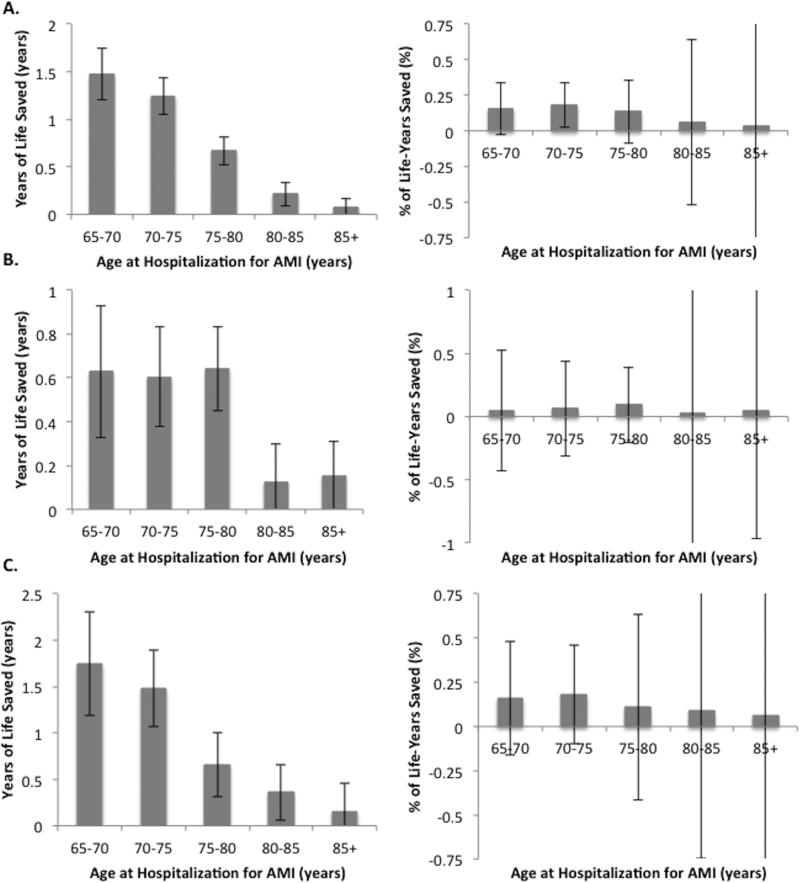
Results: Survival for recipients and non-recipients of the 5 guideline-based therapies diverged early after admission and continued to diverge during 17-year follow-up. Receipt of aspirin, beta-blockers, and acute reperfusion therapy on admission was associated with longer life expectancy of 0.78 (standard error [SE]: 0.05), 0.55 (SE: 0.06), and 1.03 (SE: 0.12) years, respectively. Patients receiving primary percutaneous coronary intervention (PCI) within 90 min lived 1.08 (SE: 0.49) years longer than patients with D2B times >90 min, and door-to-needle (D2N) times ≤30 min were associated with 0.55 (SE: 0.12) more years of life. A dose-response relationship was observed between longer D2B and D2N times and shorter life expectancy after AMI.
Conclusions: Guideline-based therapy for AMI admission is associated with both early and late survival benefits, and results in meaningful gains in life expectancy and large numbers of years of life saved in elderly patients.
Keywords: acute myocardial infarction; elderly; guidelines; life expectancy; survival.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Closing the Gap Between Clinical Trials and Practice: A Global Imperative.J Am Coll Cardiol. 2016 May 24;67(20):2392-2394. doi: 10.1016/j.jacc.2016.04.002. J Am Coll Cardiol. 2016. PMID: 27199063 No abstract available.
References
-
- Oakbrook IL. Core Measure Sets. The Joint Commission; 2014. [March 12, 2014]. Available at: http://www.jointcommission.org/core_measure_sets.aspx.
-
- Krumholz HM, Anderson JL, Brooks NH, et al. ACC/AHA clinical performance measures for adults with ST-elevation and non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Circulation. 2006;113:732–61. - PubMed
-
- Process of Care Measures. Centers for Medicare and Medicaid Services (CMS); Baltimore, M.D.: 2013. [March 12, 2014]. Available at: http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instr....
-
- Metoprolol in acute myocardial infarction (MIAMI) A randomised placebo-controlled international trial. The MIAMI Trial Research Group. Eur Heart J. 1985;6:199–226. - PubMed
-
- Randomised trial of intravenous atenolol among 16,027 cases of suspected acute myocardial infarction: ISIS-1. First International Study of Infarct Survival Collaborative Group. Lancet. 1986;2:57–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
