

Do Visual and Vestibular Inputs Compensate for Somatosensory Loss in the Perception of Spatial Orientation? Insights from a Deafferented Patient
- PMID: 27199704
- PMCID: PMC4848302
- DOI: 10.3389/fnhum.2016.00181
Do Visual and Vestibular Inputs Compensate for Somatosensory Loss in the Perception of Spatial Orientation? Insights from a Deafferented Patient
Abstract
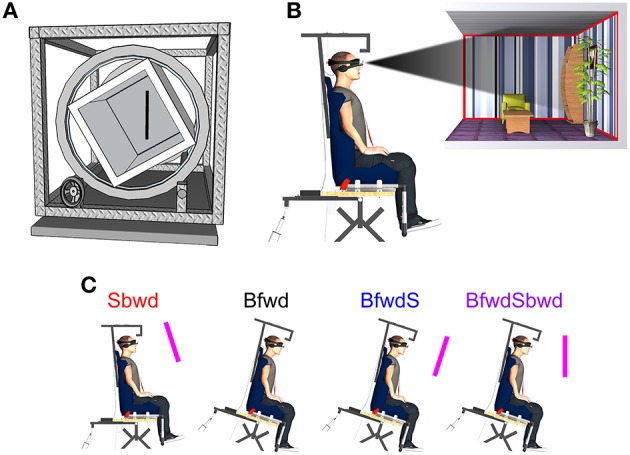
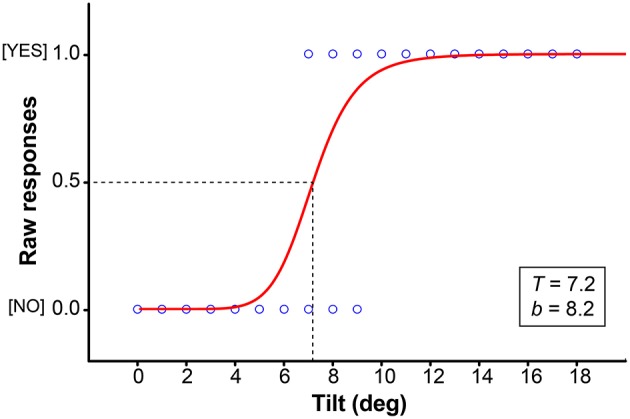
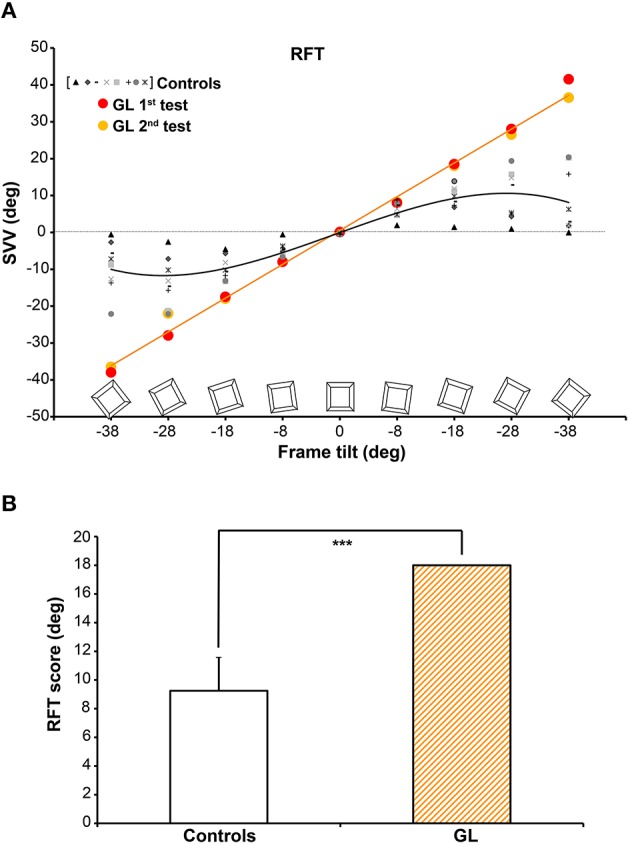
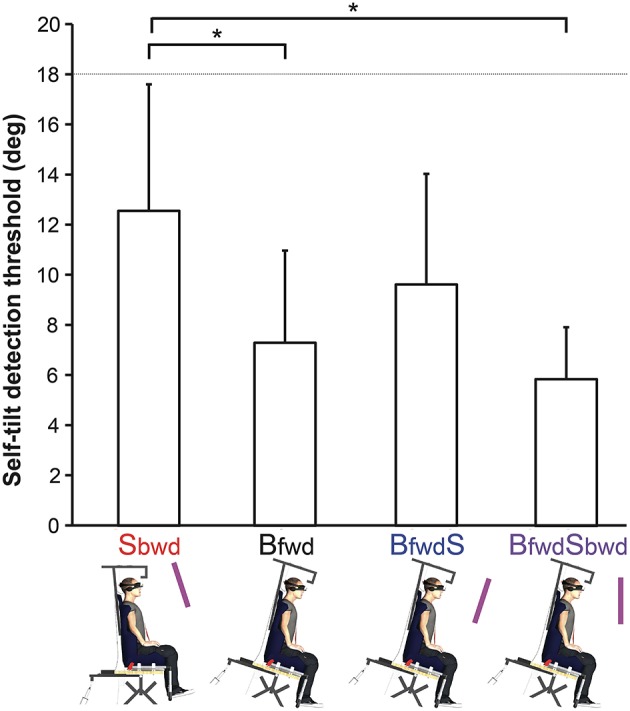
The present study aimed at investigating the consequences of a massive loss of somatosensory inputs on the perception of spatial orientation. The occurrence of possible compensatory processes for external (i.e., object) orientation perception and self-orientation perception was examined by manipulating visual and/or vestibular cues. To that aim, we compared perceptual responses of a deafferented patient (GL) with respect to age-matched Controls in two tasks involving gravity-related judgments. In the first task, subjects had to align a visual rod with the gravitational vertical (i.e., Subjective Visual Vertical: SVV) when facing a tilted visual frame in a classic Rod-and-Frame Test. In the second task, subjects had to report whether they felt tilted when facing different visuo-postural conditions which consisted in very slow pitch tilts of the body and/or visual surroundings away from vertical. Results showed that, much more than Controls, the deafferented patient was fully dependent on spatial cues issued from the visual frame when judging the SVV. On the other hand, the deafferented patient did not rely at all on visual cues for self-tilt detection. Moreover, the patient never reported any sensation of tilt up to 18° contrary to Controls, hence showing that she did not rely on vestibular (i.e., otoliths) signals for the detection of very slow body tilts either. Overall, this study demonstrates that a massive somatosensory deficit substantially impairs the perception of spatial orientation, and that the use of the remaining sensory inputs available to a deafferented patient differs regarding whether the judgment concerns external vs. self-orientation.
Keywords: body tilt; deafferented patient; multisensory integration; spatial orientation.
Figures
Similar articles
-
How do visual and postural cues combine for self-tilt perception during slow pitch rotations?Acta Psychol (Amst). 2014 Nov;153:51-9. doi: 10.1016/j.actpsy.2014.09.005. Epub 2014 Oct 6. Acta Psychol (Amst). 2014. PMID: 25299446
-
Dissociating vestibular and somatosensory contributions to spatial orientation.J Neurophysiol. 2016 Jul 1;116(1):30-40. doi: 10.1152/jn.00056.2016. Epub 2016 Apr 13. J Neurophysiol. 2016. PMID: 27075537 Free PMC article.
-
Young and Older Adults Differ in Integration of Sensory Cues for Vertical Perception.J Aging Res. 2020 Jul 31;2020:8284504. doi: 10.1155/2020/8284504. eCollection 2020. J Aging Res. 2020. PMID: 32802506 Free PMC article.
-
The interaction of otolith and proprioceptive information in the perception of verticality. The effects of labyrinthine and CNS disease.Ann N Y Acad Sci. 1999 May 28;871:324-33. doi: 10.1111/j.1749-6632.1999.tb09195.x. Ann N Y Acad Sci. 1999. PMID: 10372082 Review.
-
Perception of Verticality and Vestibular Disorders of Balance and Falls.Front Neurol. 2019 Apr 3;10:172. doi: 10.3389/fneur.2019.00172. eCollection 2019. Front Neurol. 2019. PMID: 31001184 Free PMC article. Review.
Cited by
-
[Pilot study: Determination of the subjective trunk vertical in upright head position].HNO. 2018 Sep;66(9):668-676. doi: 10.1007/s00106-018-0528-z. HNO. 2018. PMID: 30022256 German.
-
Body orientation contributes to modelling the effects of gravity for target interception in humans.J Physiol. 2019 Apr;597(7):2021-2043. doi: 10.1113/JP277469. Epub 2019 Feb 6. J Physiol. 2019. PMID: 30644996 Free PMC article.
-
Where is my hand in space? The internal model of gravity influences proprioception.Biol Lett. 2021 Jun;17(6):20210115. doi: 10.1098/rsbl.2021.0115. Epub 2021 Jun 2. Biol Lett. 2021. PMID: 34062087 Free PMC article.
-
The Effect of Cognitive Resource Competition Due to Dual-Tasking on the Irregularity and Control of Postural Movement Components.Entropy (Basel). 2019 Jan 15;21(1):70. doi: 10.3390/e21010070. Entropy (Basel). 2019. PMID: 33266786 Free PMC article.
-
Both whole-body rotation and visual flow induce cardiovascular autonomic response in human, but visual response is overridden by vestibular stimulation.Sci Rep. 2023 Mar 14;13(1):4191. doi: 10.1038/s41598-023-31431-z. Sci Rep. 2023. PMID: 36918631 Free PMC article.
References
-
- Aoki M., Ito Y., Burchill P., Brookes G. B., Gresty M. A. (1999). Tilted perception of the subjective ≪ upright ≫ in unilateral loss of vestibular function. Am. J. Otol. 20, 741–747. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources