

Colorectal cancer screening: Estimated future colonoscopy need and current volume and capacity
- PMID: 27200481
- PMCID: PMC5559728
- DOI: 10.1002/cncr.30070
Colorectal cancer screening: Estimated future colonoscopy need and current volume and capacity
Erratum in
-
Erratum.Cancer. 2017 Oct 1;123(19):3857. doi: 10.1002/cncr.30890. Epub 2017 Jul 25. Cancer. 2017. PMID: 28940328 No abstract available.
Abstract
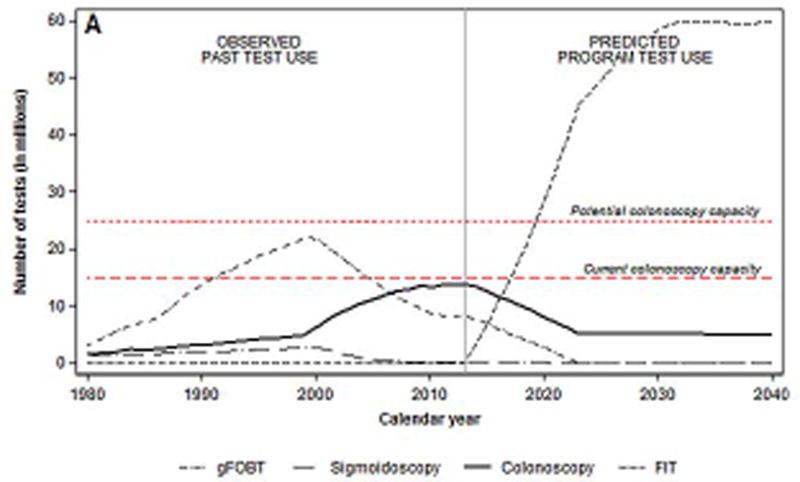
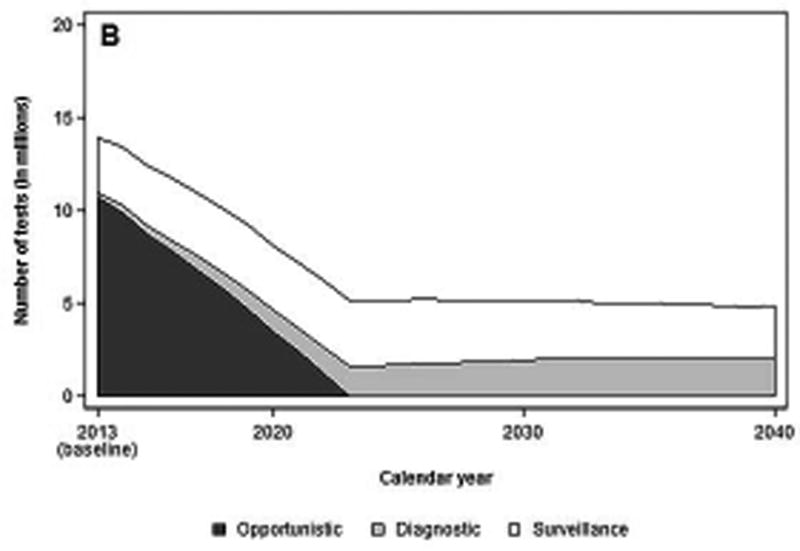
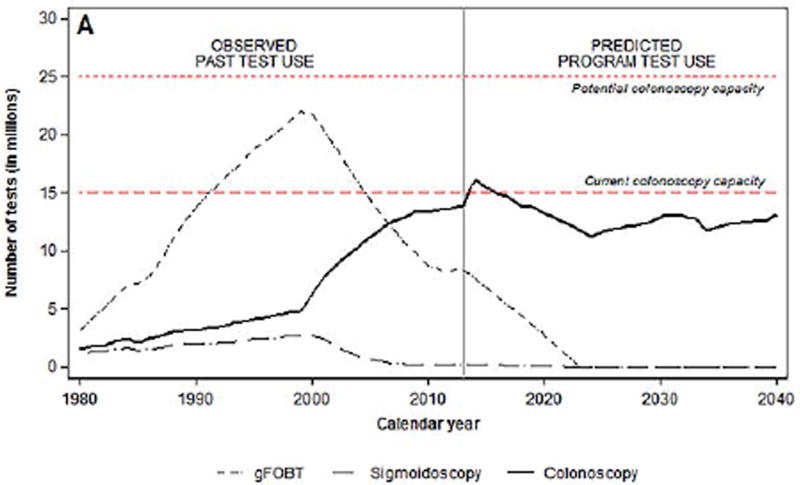
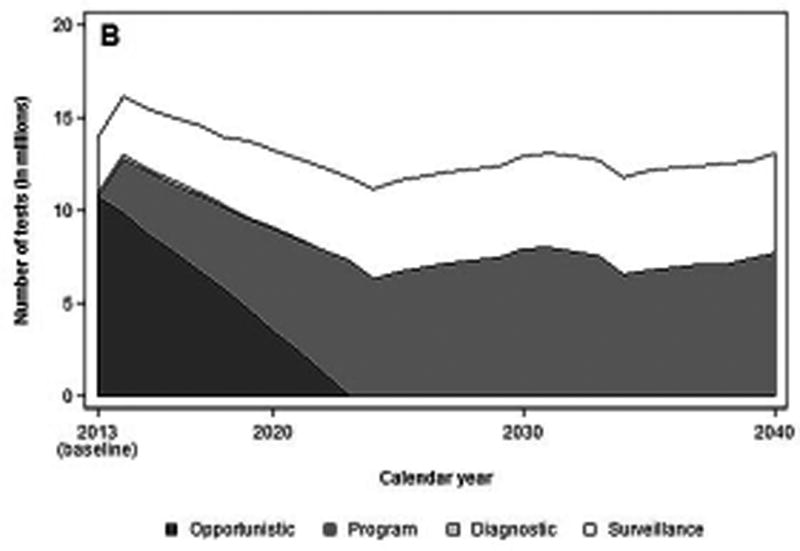
Background: In 2014, a national campaign was launched to increase colorectal cancer (CRC) screening rates in the United States to 80% by 2018; it is unknown whether there is sufficient colonoscopy capacity to reach this goal. This study estimated the number of colonoscopies needed to screen 80% of the eligible population with fecal immunochemical testing (FIT) or colonoscopy and determined whether there was sufficient colonoscopy capacity to meet the need.
Methods: The Microsimulation Screening Analysis-Colon model was used to simulate CRC screening test use in the United States (2014-2040); the implementation of a national screening program in 2014 with FIT or colonoscopy with 80% participation was assumed. The 2012 Survey of Endoscopic Capacity (SECAP) estimated the number of colonoscopies that were performed and the number that could be performed.
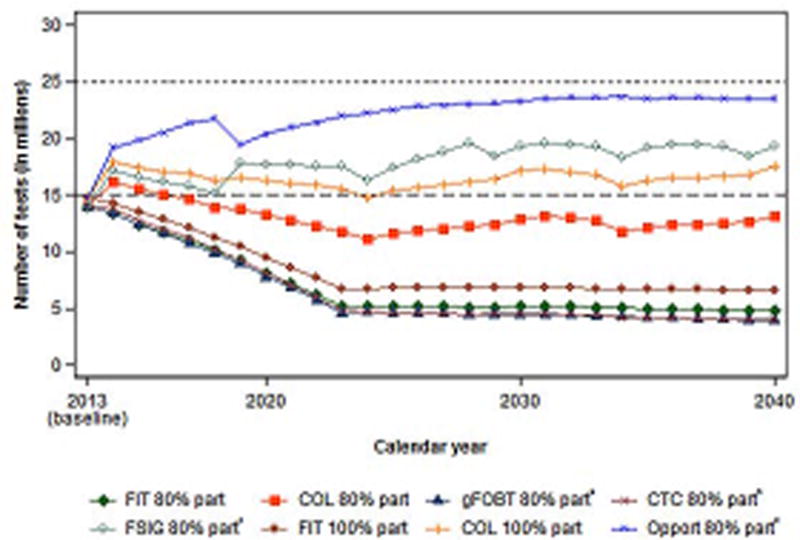
Results: If a national screening program started in 2014, by 2024, approximately 47 million FIT procedures and 5.1 million colonoscopies would be needed annually to screen the eligible population with a program using FIT as the primary screening test; approximately 11 to 13 million colonoscopies would be needed annually to screen the eligible population with a colonoscopy-only screening program. According to the SECAP survey, an estimated 15 million colonoscopies were performed in 2012, and an additional 10.5 million colonoscopies could be performed.
Conclusions: The estimated colonoscopy capacity is sufficient to screen 80% of the eligible US population with FIT, colonoscopy, or a mix of tests. Future analyses should take into account the geographic distribution of colonoscopy capacity. Cancer 2016;122:2479-86. © 2016 American Cancer Society.
Keywords: capacity; colonoscopy; colorectal cancer screening.
© 2016 American Cancer Society.
Conflict of interest statement
Figures
References
-
- U.S. Preventive Service Task Force. Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008;149:627–37. - PubMed
-
- National Center for Health Statistics. Data file documentation, National Health Interview Survey, 2010 (machine readable data file and documentation) Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention; 2014.
-
- Fedewa SA, Ma J, Sauer AG, et al. How many individuals will need to be screened to increase colorectal cancer screening prevalence to 80% by 2018? Cancer. 2015;121:4258–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
