

Bioengineered human acellular vessels for dialysis access in patients with end-stage renal disease: two phase 2 single-arm trials
- PMID: 27203778
- PMCID: PMC4915925
- DOI: 10.1016/S0140-6736(16)00557-2
Bioengineered human acellular vessels for dialysis access in patients with end-stage renal disease: two phase 2 single-arm trials
Abstract
Background: For patients with end-stage renal disease who are not candidates for fistula, dialysis access grafts are the best option for chronic haemodialysis. However, polytetrafluoroethylene arteriovenous grafts are prone to thrombosis, infection, and intimal hyperplasia at the venous anastomosis. We developed and tested a bioengineered human acellular vessel as a potential solution to these limitations in dialysis access.
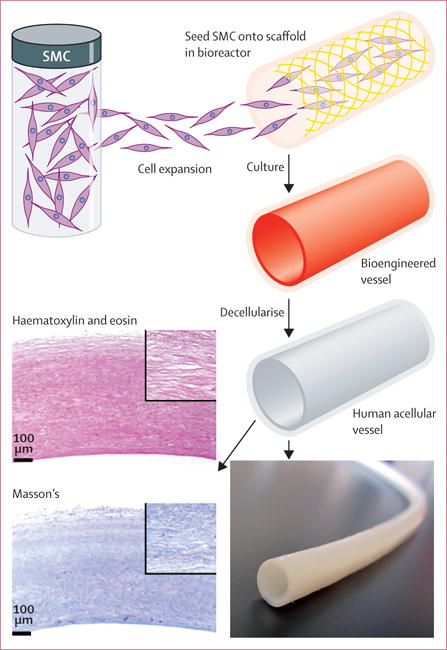
Methods: We did two single-arm phase 2 trials at six centres in the USA and Poland. We enrolled adults with end-stage renal disease. A novel bioengineered human acellular vessel was implanted into the arms of patients for haemodialysis access. Primary endpoints were safety (freedom from immune response or infection, aneurysm, or mechanical failure, and incidence of adverse events), and efficacy as assessed by primary, primary assisted, and secondary patencies at 6 months. All patients were followed up for at least 1 year, or had a censoring event. These trials are registered with ClinicalTrials.gov, NCT01744418 and NCT01840956.
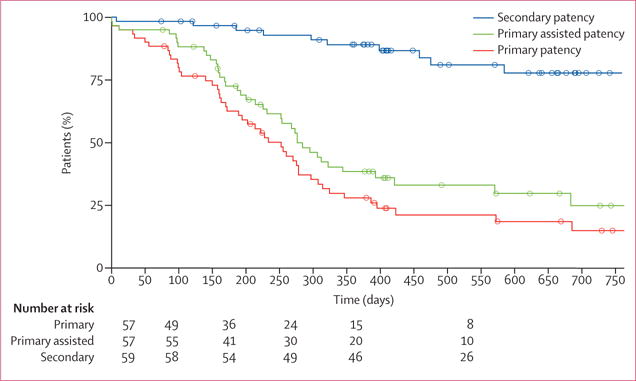
Findings: Human acellular vessels were implanted into 60 patients. Mean follow-up was 16 months (SD 7·6). One vessel became infected during 82 patient-years of follow-up. The vessels had no dilatation and rarely had post-cannulation bleeding. At 6 months, 63% (95% CI 47-72) of patients had primary patency, 73% (57-81) had primary assisted patency, and 97% (85-98) had secondary patency, with most loss of primary patency because of thrombosis. At 12 months, 28% (17-40) had primary patency, 38% (26-51) had primary assisted patency, and 89% (74-93) had secondary patency.
Interpretation: Bioengineered human acellular vessels seem to provide safe and functional haemodialysis access, and warrant further study in randomised controlled trials.
Funding: Humacyte and US National Institutes of Health.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
LEN, AJP, HLP, and JHL own stock or stock options in Humacyte. AJP and MHG work as consultants for Humacyte. The other authors declare no competing interests.
Figures
Comment in
-
Bioengineered vascular grafts off the shelf.Lancet. 2016 May 14;387(10032):1976-8. doi: 10.1016/S0140-6736(16)30180-5. Lancet. 2016. PMID: 27203754 No abstract available.
-
Dialysis: Bioengineered vessels for dialysis access: soon to be a reality?Nat Rev Nephrol. 2016 Sep;12(9):516-7. doi: 10.1038/nrneph.2016.119. Epub 2016 Aug 1. Nat Rev Nephrol. 2016. PMID: 27477493 No abstract available.
References
-
- Roy-Chaudhury P, Kelly BS, Miller MA, et al. Venous neointimal hyperplasia in polytetrafluoroethylene dialysis grafts. Kidney Int. 2001;59:2325–34. - PubMed
-
- Schon D, Blume SW, Neibauer K, Hollenbeak CS, de Lissovoy G. Increasing the use of arteriovenous fistula in hemodialysis: economic benefits and economic barriers. Clin J Am Soc Nephrol. 2007;2:268–76. - PubMed
-
- Haskal ZJ, Trerotola S, Dolmatch B, et al. Stent graft versus balloon angioplasty for failing dialysis-access grafts. N Engl J Med. 2010;362:494–503. - PubMed
-
- Akoh JA, Patel N. Infection of hemodialysis arteriovenous grafts. J Vasc Access. 2010;11:155–58. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
