

Acute heart failure with and without acute coronary syndrome: clinical correlates and prognostic impact (From the HEARTS registry)
- PMID: 27206336
- PMCID: PMC4875586
- DOI: 10.1186/s12872-016-0267-6
Acute heart failure with and without acute coronary syndrome: clinical correlates and prognostic impact (From the HEARTS registry)
Abstract
Background: Little is know about the outcomes of acute heart failure (AHF) with acute coronary syndrome (ACS-AHF), compared to those without ACS (NACS-AHF).
Methods: We conducted a prospective registry of AHF patients involving 18 hospitals in Saudi Arabia between October 2009 and December 2010. In this sub-study, we compared the clinical correlates, management and hospital course, as well as short, and long-term outcomes between AHF patients with and without ACS.
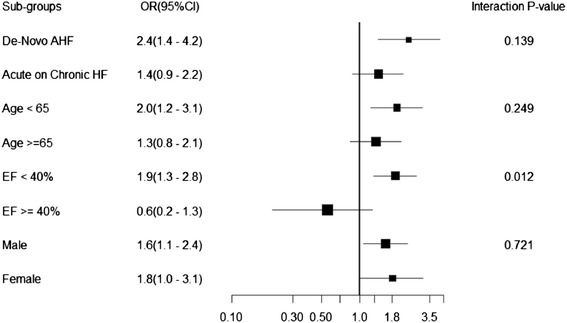
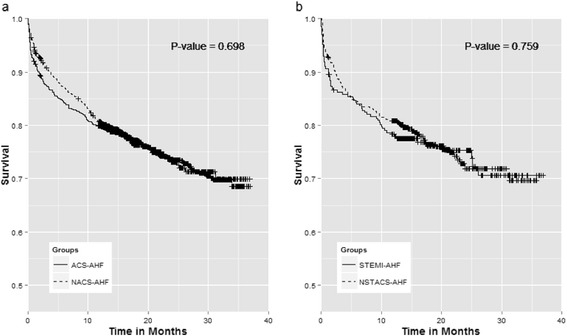
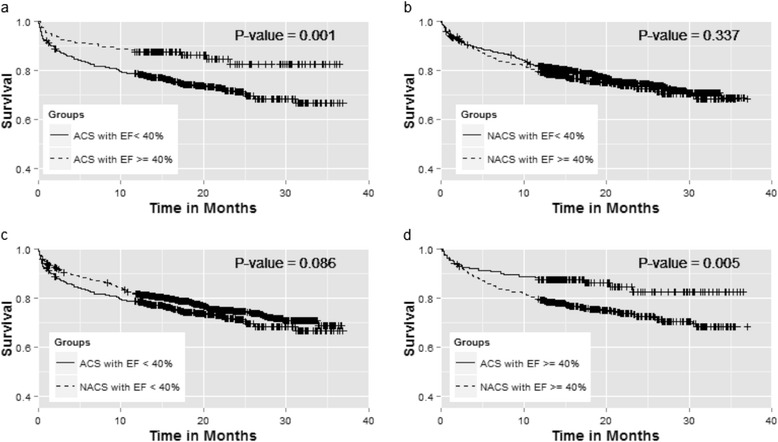
Results: Of the 2609 AHF patients enrolled, 27.8 % presented with ACS. Compared to NACS-AHF patients, ACS-AHF patients were more likely to be old males (Mean age = 62.7 vs. 60.8 years, p = 0.003, and 73.8 % vs. 62.7 %, p < 0.001, respectively), and to present with De-novo heart failure (56.6 % vs. 28.1 %, p < 0.001). Additionally they were more likely to have history of ischemic heart disease, diabetes, dyslipidemia, and less likely to have chronic kidney disease (p < 0.001 for all comparisons). The prevalence of severe LV systolic dysfunction (EF < 30 %) was higher in ACS-AHF patients. During hospital stay, ACS-AHF patients were more likely to develop shock (p < 0.001), recurrent heart failure (p = 0.02) and needed more mechanical ventilation (p < 0.001). β blockers and Angiotensin Converting Enzyme inhibitors were used more often in ACS-AHF patients (p = 0.001 and, p = 0.004 respectively). ACS- AHF patients underwent more coronary angiography and had higher prevalence of multi-vessel coronary artery disease (p < 0.001 for all comparisons). The unadjusted hospital and one-month mortality were higher in ACS-AHF patients (OR = 1.6 (1.2-2.2), p = 0.003 and 1.4 (1.0-1.9), p = 0.026 respectively). A significant interaction existed between the level of left ventricular ejection fraction and ACS-AHF status. After adjustment, ACS-AHF status was only significantly associated with hospital mortality (OR = 1.6 (1.1-2.4), p = 0.019). The three-years survival following hospital discharge was not different between the two groups.
Conclusion: AHF patients presenting with ACS had worse hospital prognosis, and an equivalent long-term survival compared to AHF patients without ACS. These findings underscore the importance of timely recognition and management of AHF patients with concomitant ACS given their distinct presentation and underlying pathophysiology compared to other AHF patients.
Keywords: Acute coronary syndrome complications/mortality/physiopathology; Heart failure complications/mortality/physiopathology; Hospital Mortality; Prospective Studies; Saudi Arabia/epidemiology.
Figures
References
-
- AlHabib KF, Elasfar AA, Alfaleh H, Kashour T, Hersi A, AlBackr H, et al. Clinical features, management, and short- and long-term outcomes of patients with acute decompensated heart failure: phase I results of the HEARTS database. Eur J Heart Fail. 2014;16(4):461–9. doi: 10.1002/ejhf.57. - DOI - PubMed
-
- Sulaiman K, Panduranga P, Al-Zakwani I, Alsheikh-Ali AA, AlHabib KF, Al-Suwaidi J, et al. Clinical characteristics, management, and outcomes of acute heart failure patients: observations from the Gulf acute heart failure registry (Gulf CARE) Eur J Heart Fail. 2015;17(4):374–84. doi: 10.1002/ejhf.245. - DOI - PubMed
-
- Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, et al. The EuroHeart Failure survey programme-- a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J. 2003;24(5):442–63. doi: 10.1016/S0195-668X(02)00823-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
