

Antiepileptic drugs' tolerability and safety--a systematic review and meta-analysis of adverse effects in dogs
- PMID: 27206489
- PMCID: PMC4875685
- DOI: 10.1186/s12917-016-0703-y
Antiepileptic drugs' tolerability and safety--a systematic review and meta-analysis of adverse effects in dogs
Abstract
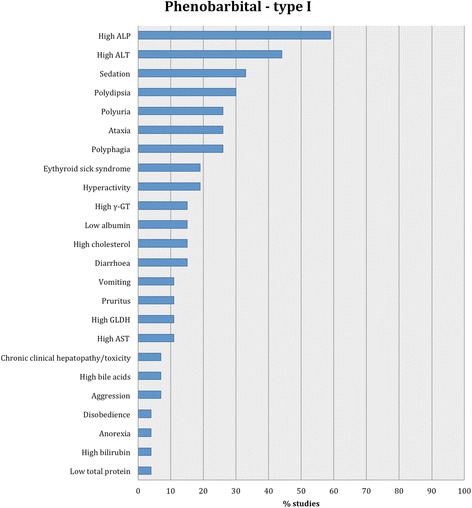
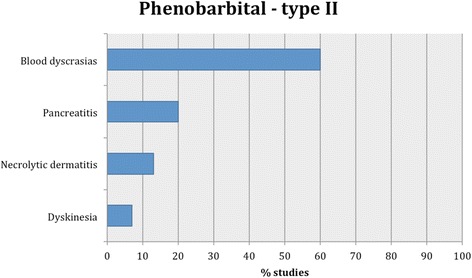
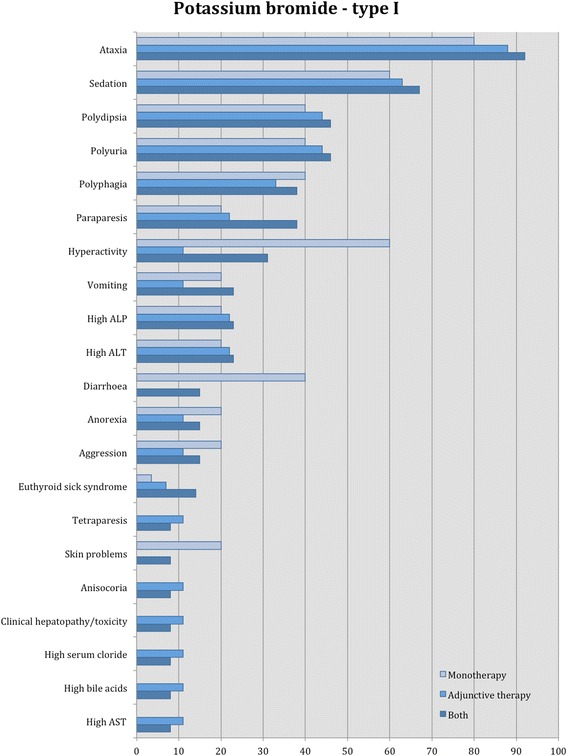
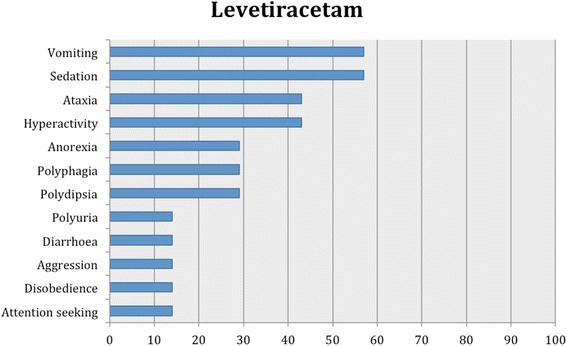
Background: The safety profile of anti-epileptic drugs (AEDs) is an important consideration for the regulatory bodies, owners and prescribing clinicians. Information on their adverse effects still remains limited. A systematic review including a meta-analytic approach was designed to evaluate existing evidence for the safety profile of AEDs in canine patients. Electronic searches of PubMed, CAB Direct and Google scholar were carried out without date or language restrictions. Conference proceedings were also searched. Peer-reviewed full-length studies reporting adverse effects of AEDs in epileptic and healthy non-epileptic dogs were included. Studies were allocated to three groups based on their design. Individual studies were evaluated based on the quality of evidence (study design, study group sizes, subject enrolment quality and overall risk of bias) and the outcome measures reported (proportion of specific adverse effects for each AED, prevalence and 95% confidence interval of the affected population in each study and comparative odds ratio of adverse effects for AEDs).
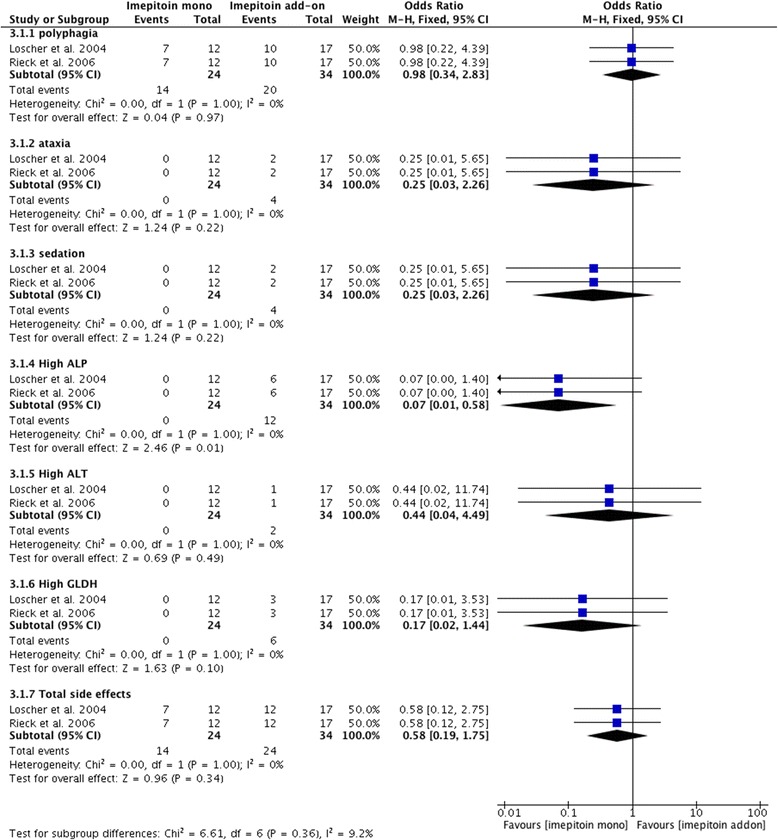
Results: Ninety studies, including six conference proceedings, reporting clinical outcomes of AEDs' adverse effects were identified. Few studies were designed as blinded randomised controlled clinical trials. Many studies included low canine populations with unclear criteria of subject enrolment and short treatment periods. Direct comparisons suggested that imepitoin and levetiracetam might have a better safety profile than phenobarbital, whilst the latter might have a better safety profile than potassium bromide. However, none of these comparisons showed a statistically significant difference. Comparisons between other AEDs were not possible as a considerable amount of studies lacked power calculations or adequate data to allow further statistical analysis. Individual AED assessments indicated that levetiracetam might be one of the safest AEDs, followed by imepitoin and then phenobarbital and potassium bromide; these findings were all supported by a strong level of evidence. The safety profile in other AEDs was variable, but weak evidence was found to permit firm conclusions or to compare their safety to other AEDs.
Conclusions: This systematic review provides objective evaluation of the most commonly used AEDs' adverse effects. Adverse effects usually appeared mild in all AEDs and subsided once doses and/or serum levels were monitored or after the AED was withdrawn. Although phenobarbital might be less safe than imepitoin and levetiracetam, there was insufficient evidence to classify it as an AED with a high risk of major adverse effects. It is important for clinicians to evaluate both AEDs' effectiveness and safety on an individual basis before the selection of the appropriate monotherapy or adjunctive AED therapy.
Keywords: Antiepileptic drugs; Canine; Epilepsy; Meta-analysis; Safety; Side effects; Systematic review.
Figures









References
-
- Baulac M: Approach of the European Medicines Agency in Development of Antiepileptic Drugs. In: Atlas of Epilepsies. edn.: Springer; 2010: 1615–1619. http://link.springer.com/referenceworkentry/10.1007/978-1-84882-128-6_243. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
