

A Randomized Controlled Trial of IVR-Based Alcohol Brief Intervention to Promote Patient-Provider Communication in Primary Care
- PMID: 27206539
- PMCID: PMC4978673
- DOI: 10.1007/s11606-016-3692-4
A Randomized Controlled Trial of IVR-Based Alcohol Brief Intervention to Promote Patient-Provider Communication in Primary Care
Abstract
Background: Brief interventions for unhealthy drinking in primary care settings are efficacious, but underutilized. Efforts to improve rates of brief intervention though provider education and office systems redesign have had limited impact. Our novel brief intervention uses interactive voice response (IVR) to provide information and advice directly to unhealthy drinkers before a physician office visit, with the goals of stimulating in-office dialogue about drinking and decreasing unhealthy drinking. This automated approach is potentially scalable for wide application.
Objective: We aimed to examine the effect of a pre-visit IVR-delivered brief alcohol intervention (IVR-BI) on patient-provider discussions of alcohol during the visit.
Design: This was a parallel group randomized controlled trial with two treatment arms: 1) IVR-BI or 2) usual care (no IVR-BI).
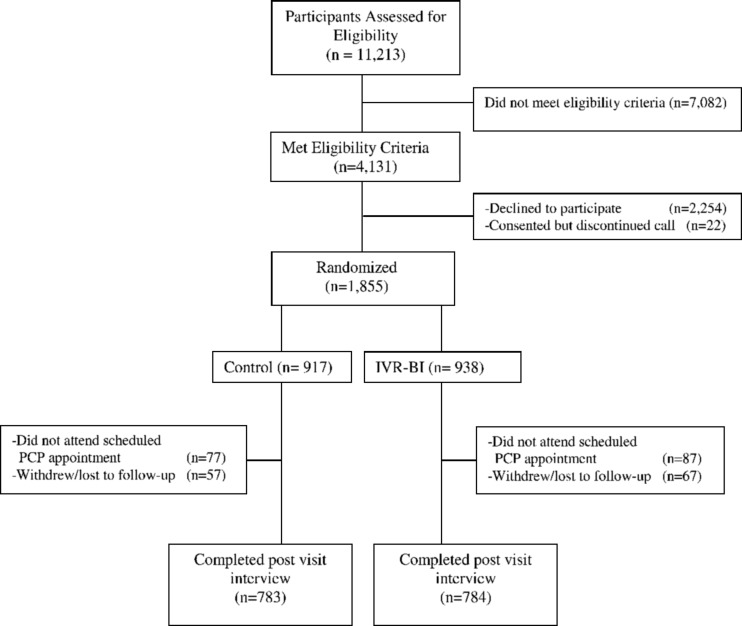
Participants: In all, 1,567 patients were recruited from eight university medical center-affiliated internal medicine and family medicine clinics.
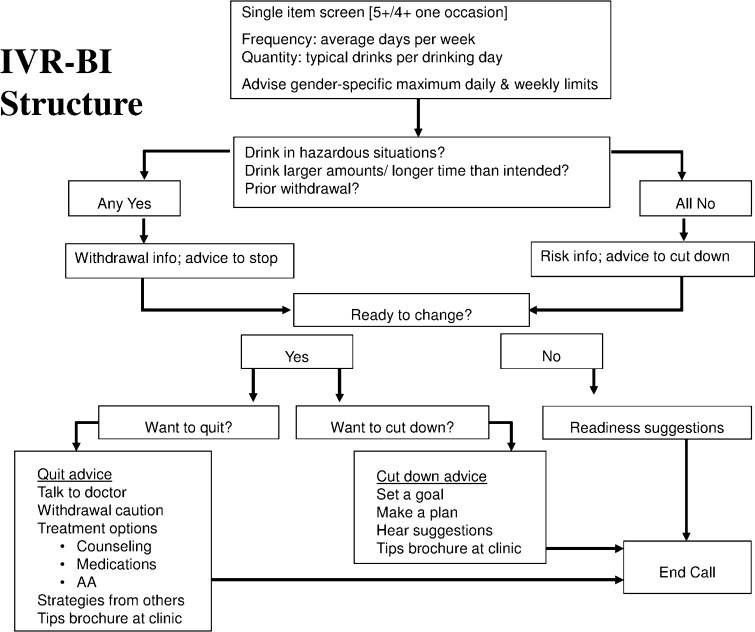
Interventions: IVR-BI is a brief alcohol intervention delivered by automated telephone. It has four components, based on the intervention steps outlined in the National Institute of Alcohol Abuse and Alcoholism guidelines for clinicians: 1) ask about alcohol use, 2) assess for alcohol use disorders, 3) advise patient to cut down or quit drinking, and 4) follow up at subsequent visits.
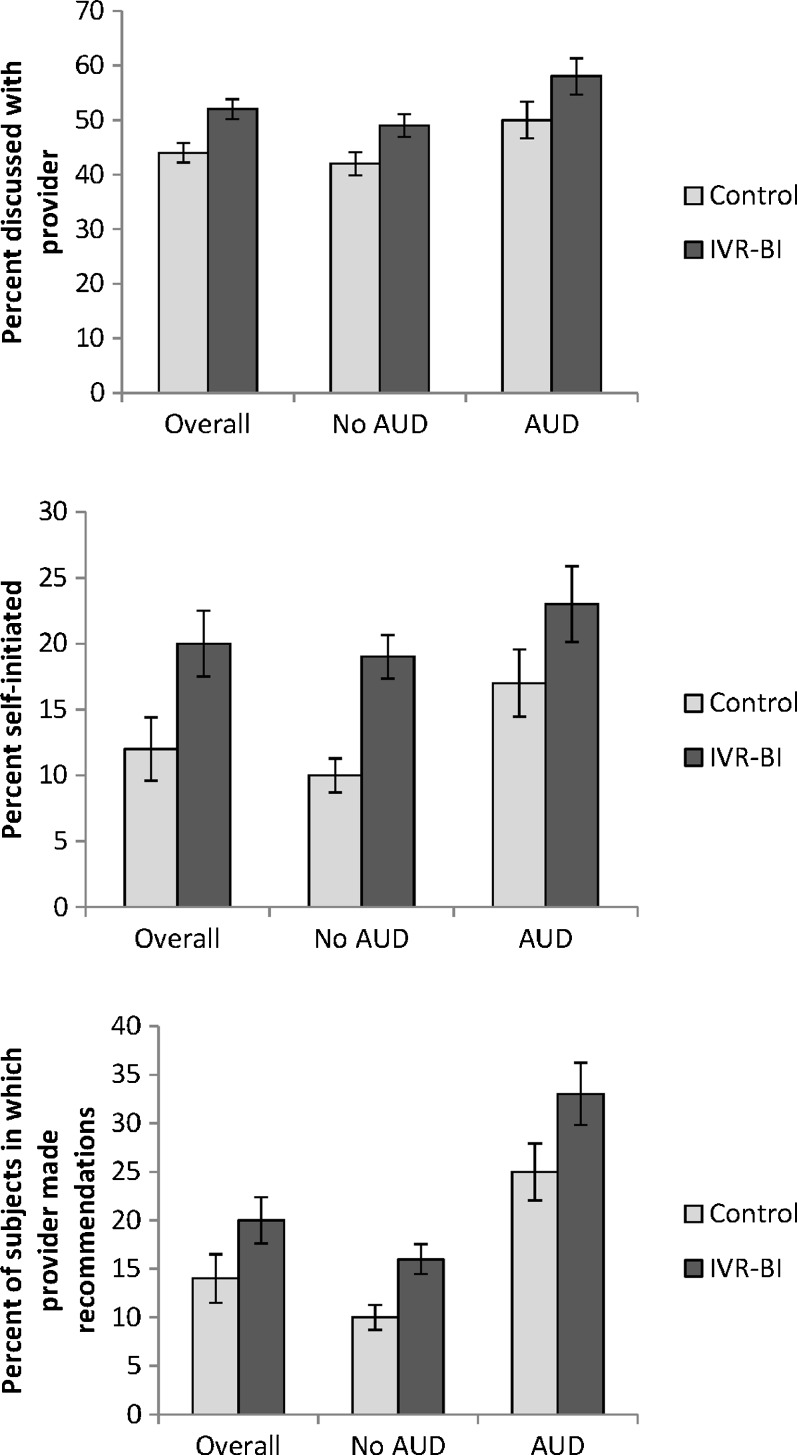
Main measures: Outcomes were patient reported: patient-provider discussion of alcohol during the visit; patient initiation of the discussion; and provider's recommendation about the patient's alcohol use.
Key results: Patients randomized to IVR-BI were more likely to have reported discussing alcohol with their provider (52 % vs. 44 %, p = 0.003), bringing up the topic themselves (20 % vs. 12 %, p < 0.001), and receiving a recommendation (20 % vs. 14 %, p < 0.001). Other predictors of outcome included baseline consumption, education, age, and alcohol use disorder diagnosis.
Conclusions: Providing automated brief interventions to patients prior to a primary care visit promotes discussion about unhealthy drinking and increases specific professional advice regarding changing drinking behavior.
Keywords: alcohol consumption; automated intervention; automated telephone; brief intervention; interactive voice response; patient engagement; physician–patient relations; primary care.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Thinking Outside the Visit: Digitally Extending the Reach of Behavioral Health.J Gen Intern Med. 2016 Sep;31(9):982-4. doi: 10.1007/s11606-016-3736-9. J Gen Intern Med. 2016. PMID: 27177912 Free PMC article. No abstract available.
References
-
- Spandorfer JM, Israel Y, Turner BJ. Primary care physicians’ views on screening and management of alcohol abuse: inconsistencies with national guidelines. J Fam Pract. 1999;48(11):899–902. - PubMed
-
- National Center on Addiction and Substance Abuse (CASA) Missed Opportunity: CASA National Survey of Primary Care Physicians and Patients on Substance Abuse. New York: Columbia University; 2000.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
