

The 30-year evolution of airway pressure release ventilation (APRV)
- PMID: 27207149
- PMCID: PMC4875584
- DOI: 10.1186/s40635-016-0085-2
The 30-year evolution of airway pressure release ventilation (APRV)
Abstract
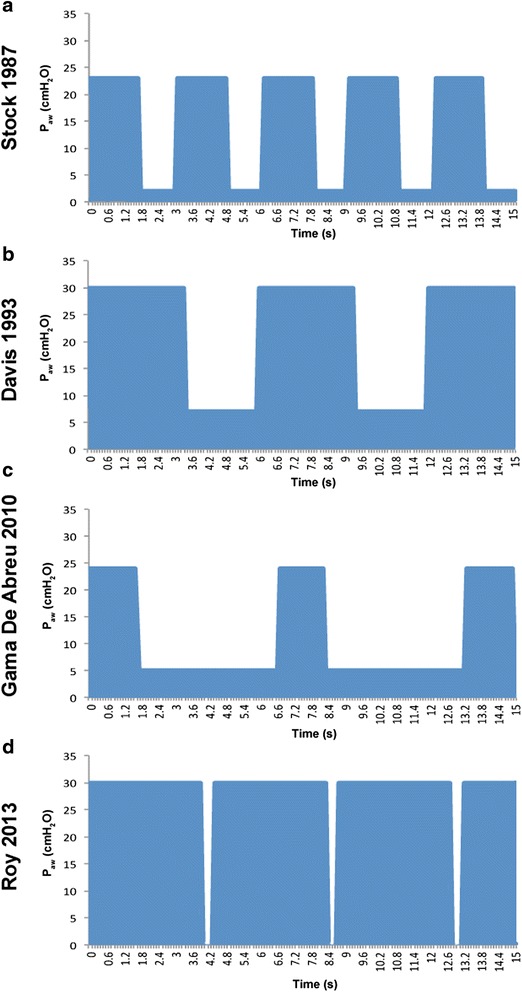
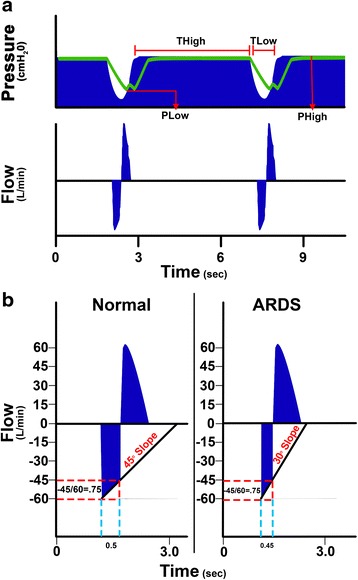
Airway pressure release ventilation (APRV) was first described in 1987 and defined as continuous positive airway pressure (CPAP) with a brief release while allowing the patient to spontaneously breathe throughout the respiratory cycle. The current understanding of the optimal strategy to minimize ventilator-induced lung injury is to "open the lung and keep it open". APRV should be ideal for this strategy with the prolonged CPAP duration recruiting the lung and the minimal release duration preventing lung collapse. However, APRV is inconsistently defined with significant variation in the settings used in experimental studies and in clinical practice. The goal of this review was to analyze the published literature and determine APRV efficacy as a lung-protective strategy. We reviewed all original articles in which the authors stated that APRV was used. The primary analysis was to correlate APRV settings with physiologic and clinical outcomes. Results showed that there was tremendous variation in settings that were all defined as APRV, particularly CPAP and release phase duration and the parameters used to guide these settings. Thus, it was impossible to assess efficacy of a single strategy since almost none of the APRV settings were identical. Therefore, we divided all APRV studies divided into two basic categories: (1) fixed-setting APRV (F-APRV) in which the release phase is set and left constant; and (2) personalized-APRV (P-APRV) in which the release phase is set based on changes in lung mechanics using the slope of the expiratory flow curve. Results showed that in no study was there a statistically significant worse outcome with APRV, regardless of the settings (F-ARPV or P-APRV). Multiple studies demonstrated that P-APRV stabilizes alveoli and reduces the incidence of acute respiratory distress syndrome (ARDS) in clinically relevant animal models and in trauma patients. In conclusion, over the 30 years since the mode's inception there have been no strict criteria in defining a mechanical breath as being APRV. P-APRV has shown great promise as a highly lung-protective ventilation strategy.
Keywords: APRV; ARDS; Lung protection; Ventilator-induced lung injury.
Figures
References
-
- Gama de Abreu M, Cuevas M, Spieth PM, Carvalho AR, Hietschold V, Stroszczynski C, Wiedemann B, Koch T, Pelosi P, Koch E. Regional lung aeration and ventilation during pressure support and biphasic positive airway pressure ventilation in experimental lung injury. Crit Care. 2010;14:R34. doi: 10.1186/cc8912. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
