

Serial cervical length determination in twin pregnancies reveals 4 distinct patterns with prognostic significance for preterm birth
- PMID: 27207277
- PMCID: PMC5045791
- DOI: 10.1016/j.ajog.2016.05.018
Serial cervical length determination in twin pregnancies reveals 4 distinct patterns with prognostic significance for preterm birth
Abstract
Background: Women with a twin gestation are at increased risk for preterm birth (PTB), and sonographic cervical length (CL) is a powerful predictor for spontaneous PTB. Obstetricians frequently monitor CL in multiple gestations; yet, the optimal method to integrate and interpret the results of serial sonographic CL has not been determined.
Objective: We sought to determine whether there are different patterns of cervical shortening in twin gestations, and whether such patterns are related to the risk of PTB.
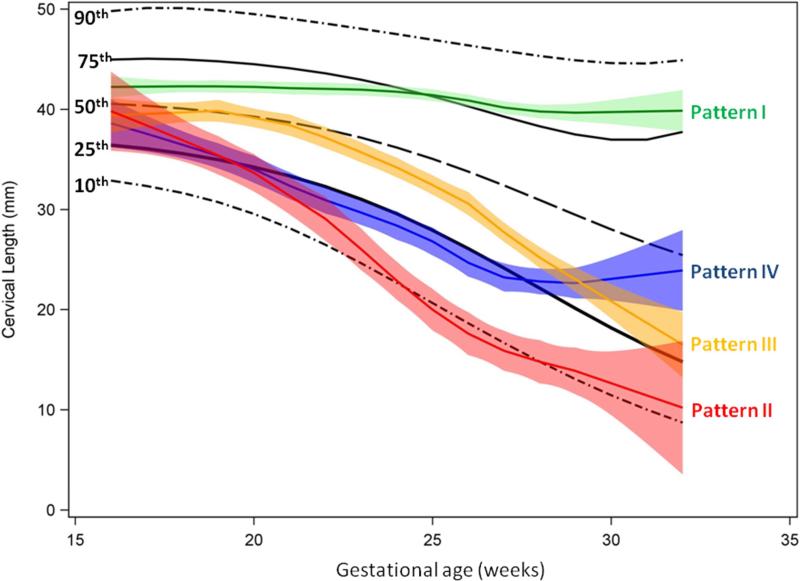
Study design: We conducted a retrospective study of all women with twins followed up in a single tertiary referral center during 2012 through 2014. All women underwent serial measurements of CL every 2-3 weeks starting from 14-18 weeks and until 28-32 weeks of gestation. Changes in CL were analyzed and classified into distinct patterns that were initially identified by visual inspection of all individual cases. Each pattern was then characterized by several parameters including information about when cervical shortening began, the rate of shortening, and whether a plateau was observed. Locally weighted regression mean profiles were generated to describe each pattern of CL over time. The association of these patterns with spontaneous PTB was determined. The specific characteristics of each pattern that further determined the risk of PTB were identified using multivariable logistic regression analysis.
Results: We studied 441 women who had a total of 2826 measurements of CL done. Overall, 4 main patterns of change in CL were identified: pattern I, stable cervix (n = 196); pattern II, early and rapid shortening (n = 18); pattern III, late shortening (n = 109); and pattern IV, early shortening with a plateau (n = 118). The rate of PTB at <34 weeks was lowest in cases of pattern I (11.7%), followed by pattern IV (14.4%) and pattern III (20.2%), and was highest for women with pattern II (44.4%) (P < .001). In cases with pattern III (late shortening), the most important factors affecting the risk of PTB were the shortening rate, the gestational age at the onset of cervical shortening, and the initial plateau of CL. In the case of pattern IV (early shortening with a plateau), it was only the new plateau at which cervical shortening stopped that was associated with the risk of PTB.
Conclusion: Changes in sonographic CL over time in twin gestations can be classified into 4 patterns, each associated with a different risk of PTB.
Keywords: biomarker; cervical ripening; longitudinal study; prediction; pregnancy; prematurity; preterm labor; ultrasound.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures




References
-
- Robertson PA, Sniderman SH, Laros RK, Jr., et al. Neonatal morbidity according to gestational age and birth weight from five tertiary care centers in the United States, 1983 through 1986. American journal of obstetrics and gynecology. 1992;166:1629–41. discussion 41-5. - PubMed
-
- Garite TJ, Clark RH, Elliott JP, Thorp JA. Twins and triplets: the effect of plurality and growth on neonatal outcome compared with singleton infants. American journal of obstetrics and gynecology. 2004;191:700–7. - PubMed
-
- Shinwell ES, Blickstein I. The risks for very low birth weight infants from multiple pregnancies. Clinics in perinatology. 2007;34:587–97, vi-vii. - PubMed
-
- Chauhan SP, Scardo JA, Hayes E, Abuhamad AZ, Berghella V. Twins: prevalence, problems, and preterm births. American journal of obstetrics and gynecology. 2010;203:305–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
