

Long-term effects of delayed-release dimethyl fumarate in multiple sclerosis: Interim analysis of ENDORSE, a randomized extension study
- PMID: 27207449
- PMCID: PMC5418934
- DOI: 10.1177/1352458516649037
Long-term effects of delayed-release dimethyl fumarate in multiple sclerosis: Interim analysis of ENDORSE, a randomized extension study
Abstract
Background: Delayed-release dimethyl fumarate (DMF) demonstrated strong efficacy and a favorable benefit-risk profile for patients with relapsing-remitting multiple sclerosis (RRMS) in phase 3 DEFINE/CONFIRM studies. ENDORSE is an ongoing long-term extension of DEFINE/CONFIRM.
Objective: We report efficacy and safety results of a 5-year interim analysis of ENDORSE (2 years DEFINE/CONFIRM; minimum 3 years ENDORSE).
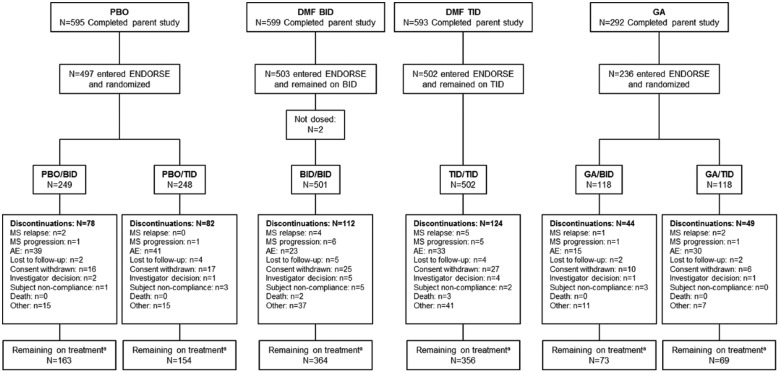
Methods: In ENDORSE, patients randomized to DMF 240 mg twice (BID) or thrice daily (TID) in DEFINE/CONFIRM continued this dosage, and those initially randomized to placebo (PBO) or glatiramer acetate (GA) were re-randomized to DMF 240 mg BID or TID.
Results: For patients continuing DMF BID (BID/BID), annualized relapse rates were 0.202, 0.163, 0.139, 0.143, and 0.138 (years 1-5, respectively) and 63%, 73%, and 88% were free of new or enlarging T2 hyperintense lesions, new T1 hypointense lesions, and gadolinium-enhanced lesions, respectively, at year 5. Adverse events (AEs; serious adverse events (SAEs)) were reported in 91% (22%; BID/BID), 95% (24%; PBO/BID), and 88% (16%; GA/BID) of the patients. One case of progressive multifocal leukoencephalopathy was reported in the setting of severe, prolonged lymphopenia.
Conclusion: Treatment with DMF was associated with continuously low clinical and magnetic resonance imaging (MRI) disease activity in patients with RRMS. These interim data demonstrate a sustained treatment benefit and an acceptable safety profile with DMF.
Keywords: DEFINE; ENDORSE; Expanded Disability Status Scale; Relapsing–remitting multiple sclerosis; delayed-release dimethyl fumarate (DMF).
Conflict of interest statement
Figures



References
-
- Oh J, O’Connor PW. Safety, tolerability, and efficacy of oral therapies for relapsing-remitting multiple sclerosis. CNS Drugs 2013; 27: 591–609. - PubMed
-
- Kretzschmar B, Pellkofer H, Weber MS. The use of oral disease-modifying therapies in multiple sclerosis. Curr Neurol Neurosci Rep 2016; 16: 38. - PubMed
-
- Fox RJ, Miller DH, Phillips JT, et al. Placebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosis. N Engl J Med 2012; 367: 1087–1097. - PubMed
-
- Gold R, Kappos L, Arnold DL, et al. Placebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosis. N Engl J Med 2012; 367: 1098–1107. - PubMed
-
- Polman CH, Reingold SC, Edan G, et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria.” Ann Neurol 2005; 58: 840–846. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
