

Toxicities of chimeric antigen receptor T cells: recognition and management
- PMID: 27207799
- PMCID: PMC4929924
- DOI: 10.1182/blood-2016-04-703751
Toxicities of chimeric antigen receptor T cells: recognition and management
Abstract
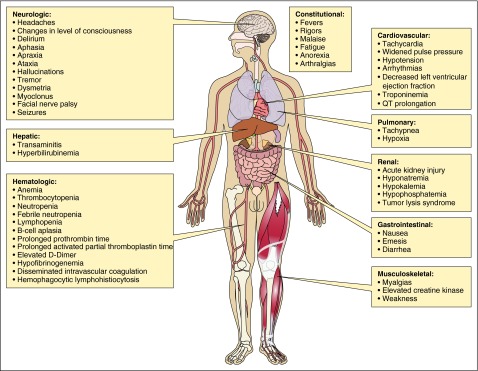
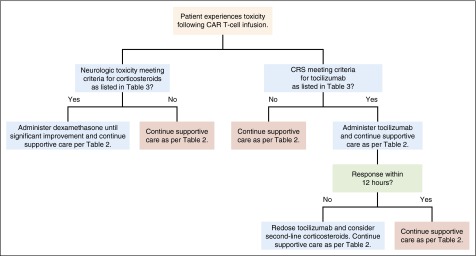
Chimeric antigen receptor (CAR) T cells can produce durable remissions in hematologic malignancies that are not responsive to standard therapies. Yet the use of CAR T cells is limited by potentially severe toxicities. Early case reports of unexpected organ damage and deaths following CAR T-cell therapy first highlighted the possible dangers of this new treatment. CAR T cells can potentially damage normal tissues by specifically targeting a tumor-associated antigen that is also expressed on those tissues. Cytokine release syndrome (CRS), a systemic inflammatory response caused by cytokines released by infused CAR T cells can lead to widespread reversible organ dysfunction. CRS is the most common type of toxicity caused by CAR T cells. Neurologic toxicity due to CAR T cells might in some cases have a different pathophysiology than CRS and requires different management. Aggressive supportive care is necessary for all patients experiencing CAR T-cell toxicities, with early intervention for hypotension and treatment of concurrent infections being essential. Interleukin-6 receptor blockade with tocilizumab remains the mainstay pharmacologic therapy for CRS, though indications for administration vary among centers. Corticosteroids should be reserved for neurologic toxicities and CRS not responsive to tocilizumab. Pharmacologic management is complicated by the risk of immunosuppressive therapy abrogating the antimalignancy activity of the CAR T cells. This review describes the toxicities caused by CAR T cells and reviews the published approaches used to manage toxicities. We present guidelines for treating patients experiencing CRS and other adverse events following CAR T-cell therapy.
Figures
References
-
- Eshhar Z, Waks T, Gross G, Schindler DG. Specific activation and targeting of cytotoxic lymphocytes through chimeric single chains consisting of antibody-binding domains and the gamma or zeta subunits of the immunoglobulin and T-cell receptors. Proc Natl Acad Sci USA. 1993;90(2):720–724. - PMC - PubMed
-
- Ghorashian S, Pule M, Amrolia P. CD19 chimeric antigen receptor T cell therapy for haematological malignancies. Br J Haematol. 2015;169(4):463–478. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
