

Death and Emergency Readmission of Infants Discharged After Interventions for Congenital Heart Disease: A National Study of 7643 Infants to Inform Service Improvement
- PMID: 27207967
- PMCID: PMC4889202
- DOI: 10.1161/JAHA.116.003369
Death and Emergency Readmission of Infants Discharged After Interventions for Congenital Heart Disease: A National Study of 7643 Infants to Inform Service Improvement
Abstract
Background: Improvements in hospital-based care have reduced early mortality in congenital heart disease. Later adverse outcomes may be reducible by focusing on care at or after discharge. We aimed to identify risk factors for such events within 1 year of discharge after intervention in infancy and, separately, to identify subgroups that might benefit from different forms of intervention.
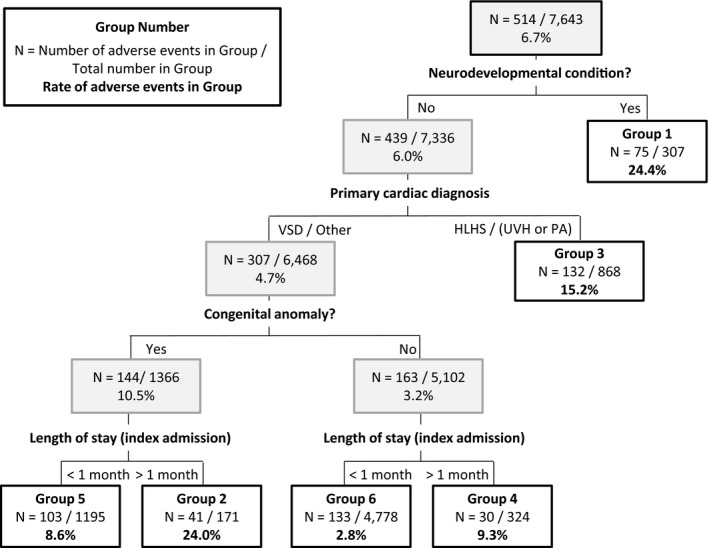
Methods and results: Cardiac procedures performed in infants between 2005 and 2010 in England and Wales from the UK National Congenital Heart Disease Audit were linked to intensive care records. Among 7976 infants, 333 (4.2%) died before discharge. Of 7643 infants discharged alive, 246 (3.2%) died outside the hospital or after an unplanned readmission to intensive care (risk factors were age, weight-for-age, cardiac procedure, cardiac diagnosis, congenital anomaly, preprocedural clinical deterioration, prematurity, ethnicity, and duration of initial admission; c-statistic 0.78 [0.75-0.82]). Of the 7643, 514 (6.7%) died outside the hospital or had an unplanned intensive care readmission (same risk factors but with neurodevelopmental condition and acquired cardiac diagnosis and without preprocedural deterioration; c-statistic 0.78 [0.75-0.80]). Classification and regression tree analysis were used to identify 6 subgroups stratified by the level (3-24%) and nature of risk for death outside the hospital or unplanned intensive care readmission based on neurodevelopmental condition, cardiac diagnosis, congenital anomaly, and duration of initial admission. An additional 115 patients died after planned intensive care admission (typically following elective surgery).
Conclusions: Adverse outcomes in the year after discharge are of similar magnitude to in-hospital mortality, warrant service improvements, and are not confined to diagnostic groups currently targeted with enhanced monitoring.
Keywords: congenital heart defects; health policy and outcomes research; pediatrics; risk model; risk stratification.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
Risk factors associated with readmission after pediatric cardiothoracic surgery.Ann Thorac Surg. 2012 Sep;94(3):865-73. doi: 10.1016/j.athoracsur.2012.04.025. Epub 2012 Jun 8. Ann Thorac Surg. 2012. PMID: 22682942
-
Ethnic-specific mortality of infants undergoing congenital heart surgery in England and Wales.Arch Dis Child. 2019 Sep;104(9):844-850. doi: 10.1136/archdischild-2018-315505. Epub 2019 Mar 1. Arch Dis Child. 2019. PMID: 30824491
-
Novel Biomarkers Improve Prediction of 365-Day Readmission After Pediatric Congenital Heart Surgery.Ann Thorac Surg. 2020 Jan;109(1):164-170. doi: 10.1016/j.athoracsur.2019.05.070. Epub 2019 Jul 16. Ann Thorac Surg. 2020. PMID: 31323208 Free PMC article.
-
Infant deaths in the UK community following successful cardiac surgery: building the evidence base for optimal surveillance, a mixed-methods study.Southampton (UK): NIHR Journals Library; 2016 May. Southampton (UK): NIHR Journals Library; 2016 May. PMID: 27252995 Free Books & Documents. Review.
-
Databases for assessing the outcomes of the treatment of patients with congenital and paediatric cardiac disease--the perspective of critical care.Cardiol Young. 2008 Dec;18 Suppl 2:130-6. doi: 10.1017/S1047951108002886. Cardiol Young. 2008. PMID: 19063783 Review.
Cited by
-
Influence of Geographic Access on Surgical Center Readmissions After Index Congenital Heart Surgery.J Pediatr. 2021 Jul;234:195-204.e3. doi: 10.1016/j.jpeds.2021.03.026. Epub 2021 Mar 24. J Pediatr. 2021. PMID: 33774056 Free PMC article.
-
Parents' Experiences of Caring for Their Child at the Time of Discharge After Cardiac Surgery and During the Postdischarge Period: Qualitative Study Using an Online Forum.J Med Internet Res. 2018 May 9;20(5):e155. doi: 10.2196/jmir.9104. J Med Internet Res. 2018. PMID: 29743157 Free PMC article.
-
Research priorities in children and adults with congenital heart disease: a James Lind Alliance Priority Setting Partnership.Open Heart. 2022 Nov;9(2):e002147. doi: 10.1136/openhrt-2022-002147. Open Heart. 2022. PMID: 36600635 Free PMC article.
-
Fetal and maternal factors are associated with mortality due to circulatory system disorders in children.Rev Saude Publica. 2019 Apr 1;53:31. doi: 10.11606/S1518-8787.2019053000793. Rev Saude Publica. 2019. PMID: 30942273 Free PMC article.
-
Inpatient costs of congenital heart surgery in China: results from the National Centre for Cardiovascular Diseases.Lancet Reg Health West Pac. 2022 Nov 8;31:100623. doi: 10.1016/j.lanwpc.2022.100623. eCollection 2023 Feb. Lancet Reg Health West Pac. 2022. PMID: 36879787 Free PMC article.
References
-
- Crowe S, Brown KL, Pagel C, Muthialu N, Cunningham D, Gibbs J, Bull C, Franklin R, Utley M, Tsang VT. Development of a diagnosis‐ and procedure‐based risk model for 30‐day outcome after pediatric cardiac surgery. J Thorac Cardiovasc Surg. 2013;145:1270–1278. - PubMed
-
- Jacobs JP, O'Brien SM, Pasquali SK, Jacobs ML, Lacour‐Gayet FG, Tchervenkov CI, Austin EH, Pizarro C, Pourmoghadam KK, Scholl FG, Welke KF, Mavroudis C. Variation in outcomes for benchmark operations: an analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. Ann Thorac Surg. 2012;92:2184–2192. - PMC - PubMed
-
- Ghanayem NS, Allen KR, Tabbutt S, Atz AM, Clabby ML, Cooper DS, Eghtesady P, Frommelt PC, Gruber PJ, Hill KD, Kaltman JR, Laussen PC, Lewis AB, Lurito KJ, Minich LL, Ohye RG, Schonbeck JV, Schwartz SM, Singh RK, Goldberg CS; Pediatric Heart Network Investigators . Interstage mortality after the Norwood procedure: results of the multicenter Single Ventricle Reconstruction trial. J Thorac Cardiovasc Surg. 2012;144:896–906. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
