

SGLT2 Inhibitors and Cardiovascular Risk: Lessons Learned From the EMPA-REG OUTCOME Study
- PMID: 27208375
- PMCID: PMC4839176
- DOI: 10.2337/dc16-0041
SGLT2 Inhibitors and Cardiovascular Risk: Lessons Learned From the EMPA-REG OUTCOME Study
Abstract
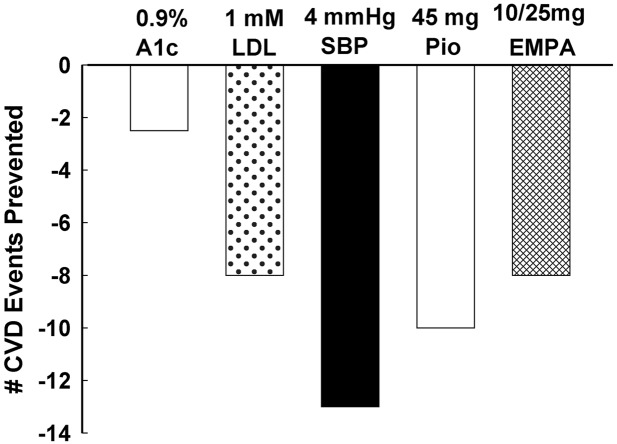
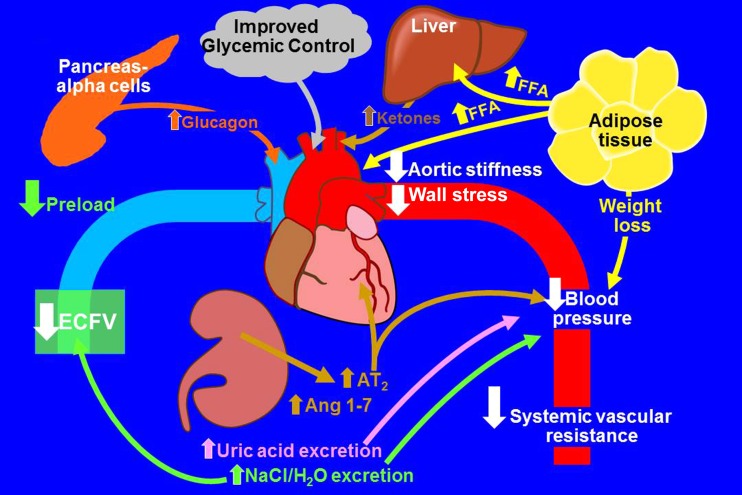
Although cardiovascular (CV) mortality is the principal cause of death in individuals with type 2 diabetes (T2DM), reduction of plasma glucose concentration has little effect on CV disease (CVD) risk. Thus, novel strategies to reduce CVD risk in T2DM patients are needed. The recently published BI 10773 (Empagliflozin) Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) study demonstrated that in T2DM patients with high CVD risk empagliflozin reduced the primary major adverse cardiac event end point (CV death, nonfatal myocardial infarction, nonfatal stroke) by 14%. This beneficial effect was driven by a 38% reduction in CV mortality with no significant decrease in nonfatal myocardial infarction or stroke. Empagliflozin also caused a 35% reduction in hospitalization for heart failure without affecting hospitalization for unstable angina. Although sodium-glucose cotransporter 2 inhibitors exert multiple metabolic benefits (decreases in HbA1c, body weight, and blood pressure and an increase in HDL cholesterol), all of which could reduce CVD risk, it is unlikely that the reduction in CV mortality can be explained by empagliflozin's metabolic effects. More likely, hemodynamic effects, specifically reduced blood pressure and decreased extracellular volume, are responsible for the reduction in CV mortality and heart failure hospitalization. In this Perspective, we will discuss possible mechanisms for these beneficial effects of empagliflozin and their implications for the care of T2DM patients.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures

References
-
- Zinman B, Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators . Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117–2128 - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837–853 - PubMed
-
- Patel A, MacMahon S, Chalmers J, et al.; ADVANCE Collaborative Group . Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560–2572 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
