

The effects of extracellular contrast agent (Gadobutrol) on the precision and reproducibility of cardiovascular magnetic resonance feature tracking
- PMID: 27209219
- PMCID: PMC4875661
- DOI: 10.1186/s12968-016-0249-y
The effects of extracellular contrast agent (Gadobutrol) on the precision and reproducibility of cardiovascular magnetic resonance feature tracking
Abstract
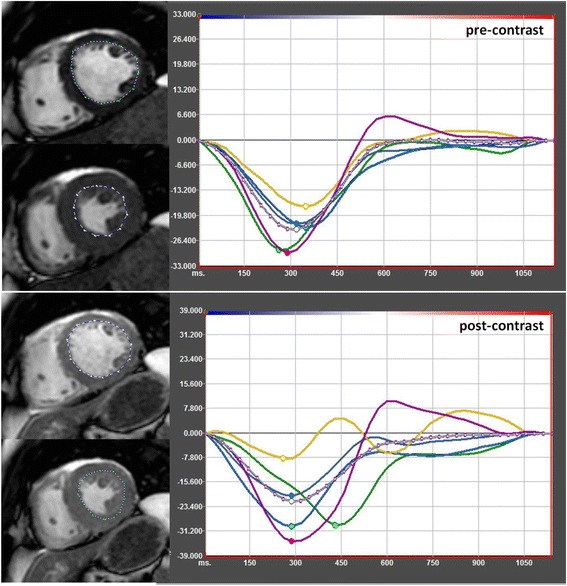
Background: Today feature tracking (FT) is considered to be a robust assessment tool in cardiovascular magnetic resonance (CMR) for strain assessment. The FT algorithm is dependent on a high contrast between blood pool and myocardium. Extracellular contrast agents decrease blood-myocardial contrast in SSFP images and thus might affect FT results. However, in a routine CMR scan, SSFP-cine images including short axis views are partly acquired after contrast agent injection. The aim of this study was to investigate the effect of extracellular contrast agent (Gadobutrol) (CA) on the precision and reproducibility of the feature tracking algorithm.
Methods: A total of 40 patient volunteers (mean age 51.2 ± 19 years; mean LVEF 61 ± 9 %) were scanned in supine position on a clinical 1.5 T MR scanner (Philips Ingenia). SSFP-cine images in midventricular short axis view (SA) as well as horizontal long axis view (HLA) were acquired before and 10-15 min after injection of a double dose Gadobutrol. FT derived systolic circumferential and longitudinal strain parameters were then calculated for pre- and post-contrast images.
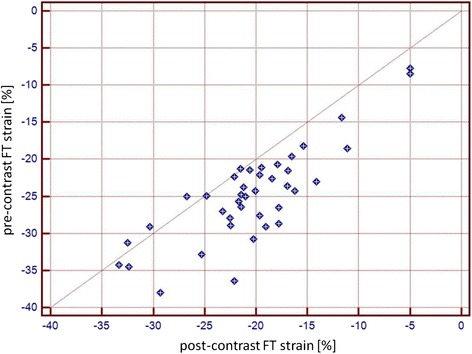
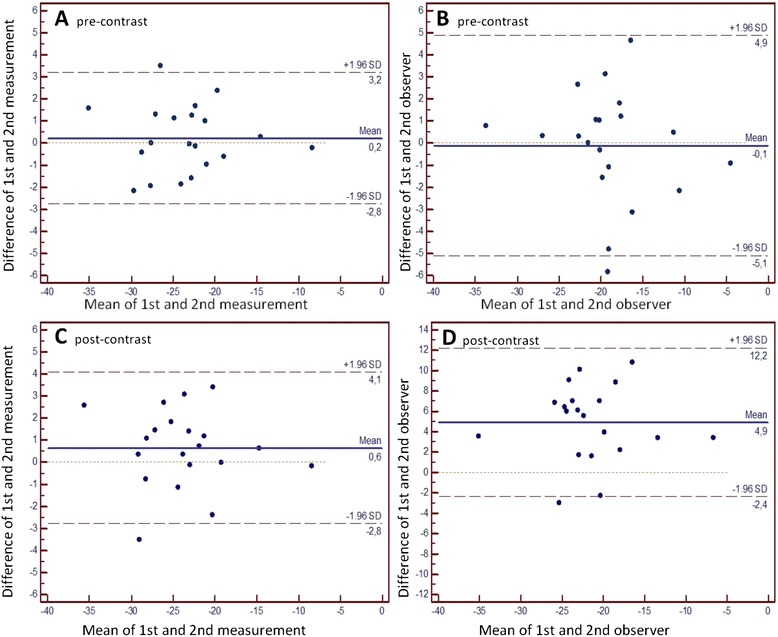
Results: FT derived midventricular peak systolic circumferential strain (PSCS) (-24.8 ± 6.4 % vs. -20.4 ± 6.3 %), apical PSCS (-28.67 ± 6.5 % vs. -24.06 ± 8.5 %), basal PSCS (-24.42 % ± 6.5 vs. -20.68 ± 7.1 %), peak systolic longitudinal strain (-19.57 ± 3.3 % vs. -17.24 ± 4.1 %), midventricular epicardial PSCS (-9.84 ± 3.4 % vs. -8.13 ± 3.4 %) , midventricular PSCS-rate (-1.52 ± 0.4 vs. -1.28 ± 0.5) and peak diastolic circumferential strain rate (1.4 ± 0.5 vs. 1.05 ± 0.5) were significantly reduced after CA application. Post CA strain assessment showed higher intra- and interobserver variability. Pre-CA: intraobserver: mean 0.21, Limits of agreement (LoA) -2.8 and 3.2; interobserver: mean 0.64, LoA -2.8 and 4.1. Post-CA: intraobserver: mean -0.11, LoA -5.1 to 4.9; interobserver: mean 4.93 LoA 2.4 to 12.2.
Conclusion: The FT algorithm is dependent on a high contrast between blood and myocardium. Post CA strain results are significantly lower and less reproducible than pre-CA strain results.
Keywords: Cardiovascular magnetic resonance; Feature tracking; Gadobutrol; Myocardial strain; Robustness.
Figures
Similar articles
-
The effect of contrast agents on left ventricular parameters calculated by a threshold-based software module: does it truly matter?Int J Cardiovasc Imaging. 2019 Sep;35(9):1683-1689. doi: 10.1007/s10554-019-01587-9. Epub 2019 Apr 29. Int J Cardiovasc Imaging. 2019. PMID: 31037474 Free PMC article.
-
The effects of flip angle optimization on the precision and reproducibility of feature tracking derived strain assessment in contrast enhanced bSSFP cine images.Eur J Radiol. 2018 May;102:9-14. doi: 10.1016/j.ejrad.2018.02.035. Epub 2018 Mar 1. Eur J Radiol. 2018. PMID: 29685551
-
Cardiovascular magnetic resonance myocardial feature tracking using a non-rigid, elastic image registration algorithm: assessment of variability in a real-life clinical setting.J Cardiovasc Magn Reson. 2017 Feb 17;19(1):24. doi: 10.1186/s12968-017-0333-y. J Cardiovasc Magn Reson. 2017. PMID: 28209163 Free PMC article.
-
Age- and gender-related normal left ventricular deformation assessed by cardiovascular magnetic resonance feature tracking.J Cardiovasc Magn Reson. 2015 Mar 10;17(1):25. doi: 10.1186/s12968-015-0123-3. J Cardiovasc Magn Reson. 2015. PMID: 25890093 Free PMC article.
-
Principles of cardiovascular magnetic resonance feature tracking and echocardiographic speckle tracking for informed clinical use.J Cardiovasc Magn Reson. 2016 Aug 26;18(1):51. doi: 10.1186/s12968-016-0269-7. J Cardiovasc Magn Reson. 2016. PMID: 27561421 Free PMC article. Review.
Cited by
-
Influence of observer experience on cardiac magnetic resonance strain measurements using feature tracking and conventional tagging.Int J Cardiol Heart Vasc. 2018 Mar 6;18:46-51. doi: 10.1016/j.ijcha.2018.02.007. eCollection 2018 Mar. Int J Cardiol Heart Vasc. 2018. PMID: 29876503 Free PMC article.
-
The effect of contrast agents on left ventricular parameters calculated by a threshold-based software module: does it truly matter?Int J Cardiovasc Imaging. 2019 Sep;35(9):1683-1689. doi: 10.1007/s10554-019-01587-9. Epub 2019 Apr 29. Int J Cardiovasc Imaging. 2019. PMID: 31037474 Free PMC article.
-
Journal of Cardiovascular Magnetic Resonance 2017.J Cardiovasc Magn Reson. 2018 Dec 28;20(1):89. doi: 10.1186/s12968-018-0518-z. J Cardiovasc Magn Reson. 2018. PMID: 30593280 Free PMC article. Review.
-
Comparison between pre- and post-contrast cardiac MRI cine images: the impact on ventricular volume and strain measurement.Int J Cardiovasc Imaging. 2023 May;39(5):1055-1064. doi: 10.1007/s10554-023-02809-x. Epub 2023 Feb 25. Int J Cardiovasc Imaging. 2023. PMID: 36840896
-
The effects of flip angle and gadolinium contrast agent on single breath-hold compressed sensing cardiac magnetic resonance cine for biventricular global strain assessment.Front Cardiovasc Med. 2024 Jan 29;11:1286271. doi: 10.3389/fcvm.2024.1286271. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38347952 Free PMC article.
References
-
- Neizel M, Korosoglou G, Lossnitzer D, et al. Impact of systolic and diastolic deformation indexes assessed by strain-encoded imaging to predict persistent severe myocardial dysfunction in patients after acute myocardial infarction at follow-up. J Am Coll Cardiol. 2010;56:1056–1062. doi: 10.1016/j.jacc.2010.02.070. - DOI - PubMed
-
- Korosoglou G, Gitsioudis G, Voss A, et al. Strain-encoded cardiac magnetic resonance during high-dose dobutamine stress testing for the estimation of cardiac outcomes: comparison to clinical parameters and conventional wall motion readings. J Am Coll Cardiol. 2011;58:1140–1149. doi: 10.1016/j.jacc.2011.03.063. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
