

Comparison of Th1/Th2 cytokine profiles between primary and secondary haemophagocytic lymphohistiocytosis
- PMID: 27209435
- PMCID: PMC4875745
- DOI: 10.1186/s13052-016-0262-7
Comparison of Th1/Th2 cytokine profiles between primary and secondary haemophagocytic lymphohistiocytosis
Abstract
Background: Haemophagocytic lymphohistiocytosis (HLH) is a life-threatening disorder of immune regulation, and HLH patients with mutations in genes including PRF1, UNC13D, STX11, STXBP2, SH2D1A, XIAP, and ITK were reported to be primary HLH. Due to the different treatment options, the differentiation between primary and secondary HLH is critical. Our previous studies have showed that a Th1/Th2 cytokine profile is diagnostic for HLH, yet the cytokine profiles between primary and secondary HLH have not been compared. The aim of the study was to test whether the Th1/Th2 cytokine profile could be used as a tool to differentiate between primary and secondary HLH.
Methods: A total of 45 hospitalized Chinese children with HLH during the period of February 2010 through September 2012 were enrolled in the study. Fifty healthy children were enrolled as controls. Primary HLH related genes were sequenced using genomic DNA samples. The Th1/Th2 cytokine levels including interferon-γ (IFN-γ), tumor necrosis factor-alpha (TNF-α), interleukin (IL)-10, IL-6, IL-4 and IL-2 were quantitatively determined by cytometric bead assay techniques.
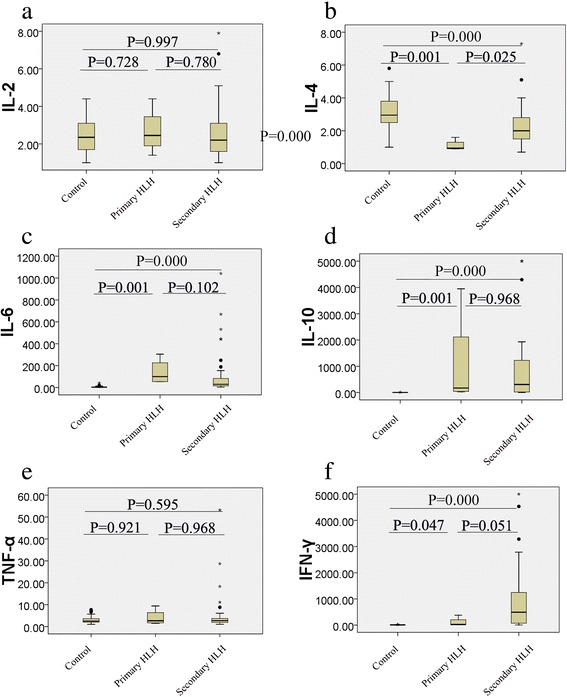
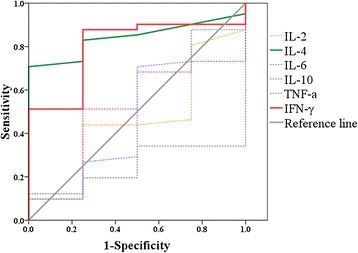
Results: Primary HLH group (n = 4) included one patient with biallelic heterozygous mutations in PRF1 gene, and three patients with hemizygous mutation in SH2D1A gene. Based on the available genetic data, the other 41 patients were classified into the secondary HLH group. When compared the cytokine levels between the two groups, IL-4 level in primary-HLH was significantly lower than that in secondary HLH (P = 0.025), while IFN-γ level in primary HLH had a tendency of statistically lower than that in secondary HLH (P = 0.051). Area under receiver operating characteristic (ROC) curves of IL-4 and IFN-γ, IL-10, TNF-α, IL-2, and IL-6 levels were 0.841, 0.799, 0.506, 0.494, 0.457, and 0.250, respectively. ROC curves showed that 1.7 pg/ml of IL-4 had sensitivity and specificity for differentiation between primary and secondary HLH as 70.7 and 100.0 %, while 433.9 pg/ml of IFN-γ had sensitivity and specificity as 51.2 and 100.0 %, respectively.
Conclusions: HLH patients with lower IL-4 and IFN-γ levels have higher possibility to be primary HLH. The cytokine profile may be used as an additional tool for the quick differential diagnosis between primary and secondary HLH.
Keywords: Cytokines; Haemophagocytic lymphohistiocytosis; Interferon-γ; Interleukin-4.
Figures
Similar articles
-
[Diagnostic significance of Th1/Th2 cytokine pattern in childhood hemophagocytic lymphohistiocytosis].Zhonghua Er Ke Za Zhi. 2011 Sep;49(9):685-9. Zhonghua Er Ke Za Zhi. 2011. PMID: 22176904 Chinese.
-
Diagnostic accuracy of a specific cytokine pattern in hemophagocytic lymphohistiocytosis in children.J Pediatr. 2012 Jun;160(6):984-90.e1. doi: 10.1016/j.jpeds.2011.11.046. Epub 2012 Jan 9. J Pediatr. 2012. PMID: 22226576
-
Early diagnostic and prognostic significance of a specific Th1/Th2 cytokine pattern in children with haemophagocytic syndrome.Br J Haematol. 2008 Oct;143(1):84-91. doi: 10.1111/j.1365-2141.2008.07298.x. Epub 2008 Jul 31. Br J Haematol. 2008. PMID: 18673367
-
Advances in hemophagocytic lymphohistiocytosis: pathogenesis, early diagnosis/differential diagnosis, and treatment.ScientificWorldJournal. 2011 Mar 22;11:697-708. doi: 10.1100/tsw.2011.62. ScientificWorldJournal. 2011. PMID: 21442147 Free PMC article. Review.
-
Rare cause of Hemophagocytic Lymphohistiocytosis due to mutation in PRF1 and SH2D1A genes in two children - a case report with a review.BMC Pediatr. 2019 Mar 8;19(1):73. doi: 10.1186/s12887-019-1444-4. BMC Pediatr. 2019. PMID: 30849948 Free PMC article. Review.
Cited by
-
Simple Evaluation of Clinical Situation and Subtypes of Pediatric Hemophagocytic Lymphohistiocytosis by Cytokine Patterns.Front Immunol. 2022 Feb 28;13:850443. doi: 10.3389/fimmu.2022.850443. eCollection 2022. Front Immunol. 2022. PMID: 35296096 Free PMC article.
-
Mechanisms of Immune Dysregulation in COVID-19 Are Different From SARS and MERS: A Perspective in Context of Kawasaki Disease and MIS-C.Front Pediatr. 2022 May 5;10:790273. doi: 10.3389/fped.2022.790273. eCollection 2022. Front Pediatr. 2022. PMID: 35601440 Free PMC article. Review.
-
A Novel Combination of Docosahexaenoic Acid, All-Trans Retinoic Acid, and 1, 25-Dihydroxyvitamin D3 Reduces T-Bet Gene Expression, Serum Interferon Gamma, and Clinical Scores but Promotes PPARγ Gene Expression in Experimental Autoimmune Encephalomyelitis.J Mol Neurosci. 2016 Dec;60(4):498-508. doi: 10.1007/s12031-016-0834-4. Epub 2016 Sep 19. J Mol Neurosci. 2016. PMID: 27647308
-
Development and Validation of 18F-FDG PET/CT-Based Multivariable Clinical Prediction Models for the Identification of Malignancy-Associated Hemophagocytic Lymphohistiocytosis.Korean J Radiol. 2022 Apr;23(4):466-478. doi: 10.3348/kjr.2021.0733. Epub 2022 Mar 8. Korean J Radiol. 2022. PMID: 35289150 Free PMC article.
-
Plasma IL-17A is increased in patients with critical MIS-C and associated to in-hospital mortality.Front Immunol. 2025 Jan 27;15:1485009. doi: 10.3389/fimmu.2024.1485009. eCollection 2024. Front Immunol. 2025. PMID: 39931580 Free PMC article.
References
-
- Xiao L, Xian Y, Dai BT, Su YC, Xiao JW, Zheng QC, et al. Clinical features and outcome analysis of 83 childhood Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis with HLH-2004 protocol. Zhonghua Xue Ye Xue Za Zhi. 2011;32(10):668–72. - PubMed
-
- Koh KN, Im HJ, Chung NG, Cho B, Kang HJ, Shin HY, et al. Clinical features, genetics, and outcome of pediatric patients with hemophagocytic lymphohistiocytosis in Korea: report of a nationwide survey from Korea Histiocytosis Working Party. Eur J Haematol. 2015;94(1):51–9. doi: 10.1111/ejh.12399. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
