

Correlation Among Hypoglycemia, Glycemic Variability, and C-Peptide Preservation After Alefacept Therapy in Patients with Type 1 Diabetes Mellitus: Analysis of Data from the Immune Tolerance Network T1DAL Trial
- PMID: 27209482
- PMCID: PMC4916002
- DOI: 10.1016/j.clinthera.2016.04.032
Correlation Among Hypoglycemia, Glycemic Variability, and C-Peptide Preservation After Alefacept Therapy in Patients with Type 1 Diabetes Mellitus: Analysis of Data from the Immune Tolerance Network T1DAL Trial
Abstract
Purpose: In natural history studies, maintenance of higher levels of C-peptide secretion (a measure of endogenous insulin production) correlates with a lower incidence of major hypoglycemic events in patients with type 1 diabetes mellitus (T1D), but it is unclear whether this is also true for drug-induced C-peptide preservation.
Methods: We analyzed hypoglycemic events and glycemic control data from the T1DAL (Inducing Remission in New-Onset T1D with Alefacept) study, a trial of alefacept in new-onset T1D, which found significant C-peptide preservation at 1 and 2 years. We performed a post hoc analysis using mixed models of the association between the meal-stimulated 4-hour C-peptide AUC (4-hour AUC) and rates of major hypoglycemia, measures of glycemic control (glycosylated hemoglobin [HbA1c]; mean glucometer readings), and variability (glucometer SDs; highest and lowest readings), and an index of partial remission (insulin dose-adjusted HbA1c[ IDAA1c]).
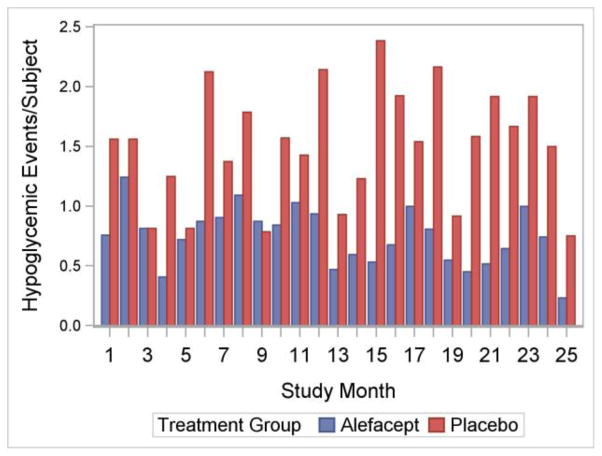
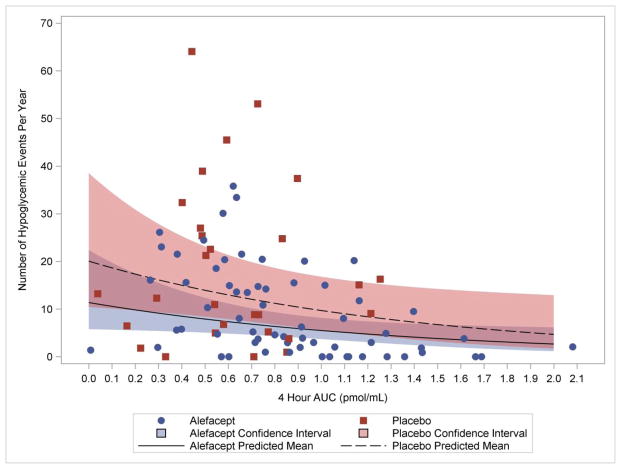
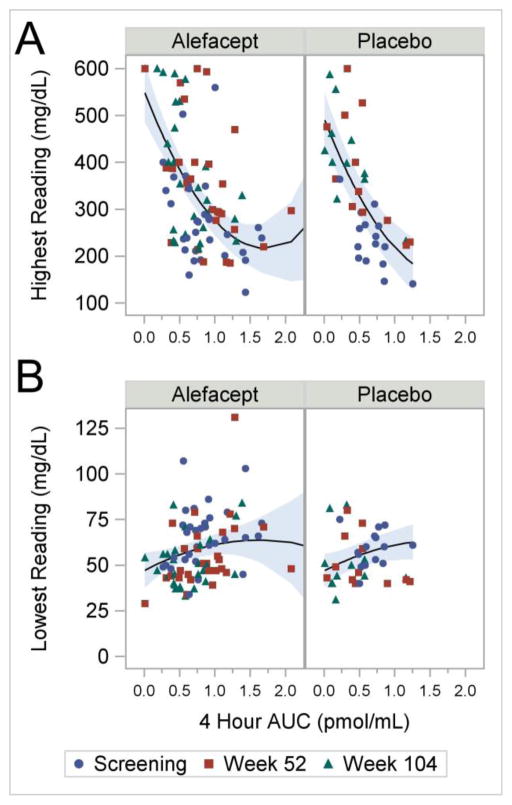
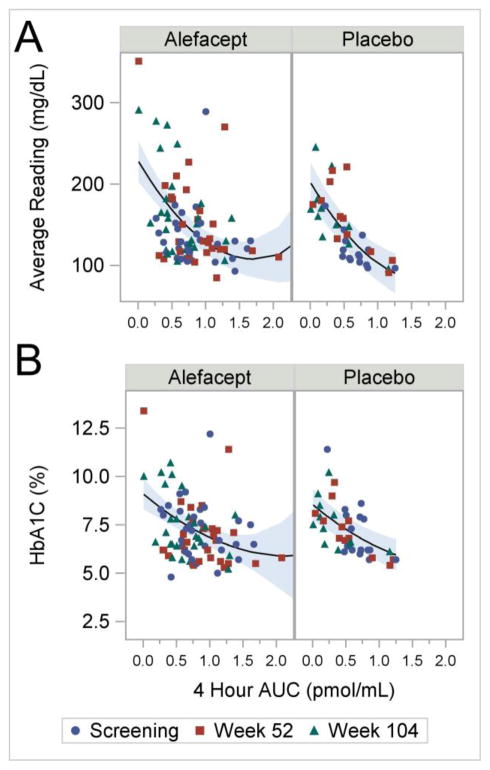
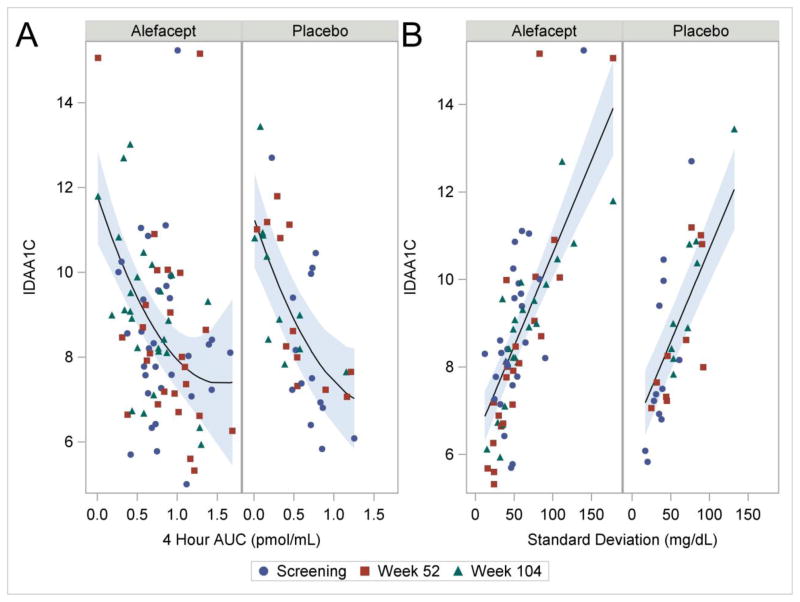
Findings: Data from 49 participants (33 in the alefacept group and 16 in the placebo group) were analyzed at baseline and 12 and 24 months. We found that the 4-hour AUC at baseline and at 1 year was a significant predictor of the number of hypoglycemic events during the ensuing 12-month interval (p = 0.030). There was a strong association between the 4-hour AUC and glucometer SDs (P < 0.001), highest readings (p < 0.001), and lowest readings (p = 0.03), all measures of glycemic variability. There was a strong inverse correlation between the 4-hour AUC and 2 measures of glycemic control: HbA1c and mean glucometer readings (both p < 0.001). There was also a strong inverse correlation between the 4-hour AUC and IDAA1c values (p < 0.001), as well as a strong correlation between IDAA1c values and glucometer SDs (p < 0.001), suggesting that reduced glycemic variability is associated with a trend toward partial remission. None of these analyses found a significant difference between the alefacept and placebo groups.
Implications: Measures of glycemic variability and control, including rates of hypoglycemia, are significantly correlated with preservation of C-peptide regardless of whether this is achieved by immune intervention with alefacept or natural variability in patients with new-onset T1D. Thus, preservation of endogenous insulin production by an immunomodulatory drug may confer clinical benefits similar to those seen in patients with higher C-peptide secretion due to slow disease progression.
Keywords: alefacept; glycemic control; hypoglycemia; immune intervention; islet function; new-onset T1d.
Copyright © 2016 Elsevier HS Journals, Inc. All rights reserved.
Figures

References
-
- Lind M, Svensson AM, Kosiborod M, et al. Glycemic control and excess mortality in type 1 diabetes. N Engl J Med. 2014;371:1972–1982. - PubMed
-
- Palta M, LeCaire T, Daniels K, Shen G, Allen C, D’Alessio D. Risk factors for hospitalization in a cohort with type 1 diabetes. Wisconsin Diabetes Registry. Am J Epidemiol. 1997;146:627–636. - PubMed
-
- Icks A, Rosenbauer J, Haastert B, Giani G. Hospitalization among diabetic children and adolescents and non-diabetic control subjects: a prospective population-based study. Diabetologia. 2001;44(Suppl 3):B87–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
