

The Society of Thoracic Surgeons Lung Cancer Resection Risk Model: Higher Quality Data and Superior Outcomes
- PMID: 27209606
- PMCID: PMC5016798
- DOI: 10.1016/j.athoracsur.2016.02.098
The Society of Thoracic Surgeons Lung Cancer Resection Risk Model: Higher Quality Data and Superior Outcomes
Erratum in
-
Corrigendum.Ann Thorac Surg. 2017 Aug;104(2):726. doi: 10.1016/j.athoracsur.2017.06.002. Ann Thorac Surg. 2017. PMID: 28734426 No abstract available.
Abstract
Background: The Society of Thoracic Surgeons (STS) creates risk-adjustment models for common cardiothoracic operations for quality improvement purposes. Our aim was to update the lung cancer resection risk model utilizing the STS General Thoracic Surgery Database (GTSD) with a larger and more contemporary cohort.
Methods: We queried the STS GTSD for all surgical resections of lung cancers from January 1, 2012, through December 31, 2014. Logistic regression was used to create three risk models for adverse events: operative mortality, major morbidity, and composite mortality and major morbidity.
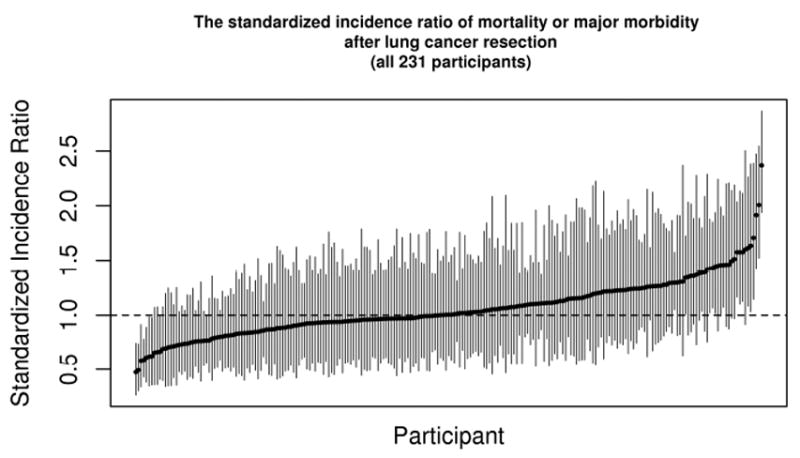
Results: In all, 27,844 lung cancer resections were performed at 231 centers; 62% (n = 17,153) were performed by thoracoscopy. The mortality rate was 1.4% (n = 401), major morbidity rate was 9.1% (n = 2,545), and the composite rate was 9.5% (n = 2,654). Predictors of mortality included age, being male, forced expiratory volume in 1 second, body mass index, cerebrovascular disease, steroids, coronary artery disease, peripheral vascular disease, renal dysfunction, Zubrod score, American Society of Anesthesiologists rating, thoracotomy approach, induction therapy, reoperation, tumor stage, and greater extent of resection (all p < 0.05). For major morbidity and the composite measure, cigarette smoking becomes a risk factor whereas stage, renal dysfunction, congestive heart failure, and cerebrovascular disease lose significance.
Conclusions: Operative mortality and complication rates are low for lung cancer resection among surgeons participating in the GTSD. Risk factors from the prior lung cancer resection model are refined, and new risk factors such as prior thoracic surgery are identified. The GTSD risk models continue to evolve as more centers report and data are audited for quality assurance.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Shahian DM, O’Brien SM, Filardo G, et al. Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1--coronary artery bypass grafting surgery. Ann Thorac Surg. 2009 Jul;88(1 Suppl):S2–22. - PubMed
-
- O’Brien SM, Shahian DM, Filardo G, et al. Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2--isolated valve surgery. Ann Thorac Surg. 2009 Jul;88(1 Suppl):S23–42. - PubMed
-
- Shahian DM, O’Brien SM, Filardo G, et al. Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 3--valve plus coronary artery bypass grafting surgery. Ann Thorac Surg. 2009 Jul;88(1 Suppl):S43–62. - PubMed
-
- Wright CD, Gaissert HA, Grab JD, et al. Predictors of prolonged length of stay after lobectomy for lung cancer: A Society of Thoracic Surgeons General Thoracic Surgery Database risk-adjustment model. Ann Thorac Surg. 2008;85:1857–65. - PubMed
-
- Kozower BD, Sheng S, O’Brien SM, et al. STS database risk models: predictors of mortality and major morbidity for lung cancer resection. Ann Thorac Surg. 2010;90:875–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
