

Comparison of Video-Assisted Thoracoscopic Surgery and Robotic Approaches for Clinical Stage I and Stage II Non-Small Cell Lung Cancer Using The Society of Thoracic Surgeons Database
- PMID: 27209613
- PMCID: PMC5198574
- DOI: 10.1016/j.athoracsur.2016.03.032
Comparison of Video-Assisted Thoracoscopic Surgery and Robotic Approaches for Clinical Stage I and Stage II Non-Small Cell Lung Cancer Using The Society of Thoracic Surgeons Database
Abstract
Background: Data from selected centers show that robotic lobectomy is safe and effective and has 30-day mortality comparable to that of video-assisted thoracoscopic surgery (VATS). However, widespread adoption of robotic lobectomy is controversial. We used The Society of Thoracic Surgeons General Thoracic Surgery (STS-GTS) Database to evaluate quality metrics for these 2 minimally invasive lobectomy techniques.
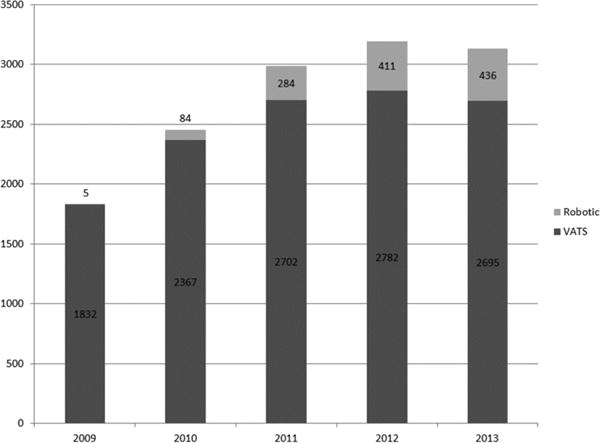
Methods: A database query for primary clinical stage I or stage II non-small cell lung cancer (NSCLC) at high-volume centers from 2009 to 2013 identified 1,220 robotic lobectomies and 12,378 VATS procedures. Quality metrics evaluated included operative morbidity, 30-day mortality, and nodal upstaging, defined as cN0 to pN1. Multivariable logistic regression was used to evaluate nodal upstaging.
Results: Patients undergoing robotic lobectomy were older, less active, and less likely to be an ever smoker and had higher body mass index (BMI) (all p < 0.05). They were also more likely to have coronary heart disease or hypertension (all p < 0.001) and to have had preoperative mediastinal staging (p < 0.0001). Robotic lobectomy operative times were longer (median 186 versus 173 minutes; p < 0.001); all other operative measurements were similar. All postoperative outcomes were similar, including complications and 30-day mortality (robotic lobectomy, 0.6% versus VATS, 0.8%; p = 0.4). Median length of stay was 4 days for both, but a higher proportion of patients undergoing robotic lobectomy had hospital stays less than 4 days (48% versus 39%; p < 0.001). Nodal upstaging overall was similar (p = 0.6) but with trends favoring VATS in the cT1b group and robotic lobectomy in the cT2a group.
Conclusions: Patients undergoing robotic lobectomy had more comorbidities and robotic lobectomy operative times were longer, but quality outcome measures, including complications, hospital stay, 30-day mortality, and nodal upstaging, suggest that robotic lobectomy and VATS are equivalent.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
References
-
- Paul S, Altorki NK, Sheng S, Lee PC, Harpole DH, Onaitis MW, et al. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg. American Association for Thoracic Surgery. 2010 Feb;139(2):366–78. - PubMed
-
- Nakata M, Saeki H, Yokoyama N, Kurita A, Takiyama W, Takashima S. Pulmonary function after lobectomy: video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg. 2000 Sep;70(3):938–41. - PubMed
-
- Whitson BA, D’Cunha J, Andrade RS, Kelly RF, Groth SS, Wu B, et al. Thoracoscopic versus thoracotomy approaches to lobectomy: differential impairment of cellular immunity. Ann Thorac Surg. 2008 Dec;86(6):1735–44. - PubMed
-
- Yim AP, Wan S, Lee TW, Arifi AA. VATS Lobectomy Reduces Cytokine Responses Compared With Conventional Surgery. Ann Thorac Surg. 2000 Jul;70(1):243–7. - PubMed
-
- Lee JG, Cho BC, Bae MK, Lee CY, Park IK, Kim DJ, et al. Thoracoscopic lobectomy is associated with superior compliance with adjuvant chemotherapy in lung cancer. Ann Thorac Surg. 2011 Feb;91(2):344–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
