

Consequences of Increasing Time to Colonoscopy Examination After Positive Result From Fecal Colorectal Cancer Screening Test
- PMID: 27211498
- PMCID: PMC5028249
- DOI: 10.1016/j.cgh.2016.05.017
Consequences of Increasing Time to Colonoscopy Examination After Positive Result From Fecal Colorectal Cancer Screening Test
Erratum in
-
Correction.Clin Gastroenterol Hepatol. 2018 May;16(5):787. doi: 10.1016/j.cgh.2018.02.023. Clin Gastroenterol Hepatol. 2018. PMID: 29678243 No abstract available.
-
Correction.Clin Gastroenterol Hepatol. 2018 Aug;16(8):1365. doi: 10.1016/j.cgh.2018.06.001. Clin Gastroenterol Hepatol. 2018. PMID: 30033180 No abstract available.
Abstract
Background & aims: Delays in diagnostic testing after a positive result from a screening test can undermine the benefits of colorectal cancer (CRC) screening, but there are few empirical data on the effects of such delays. We used microsimulation modeling to estimate the consequences of time to colonoscopy after a positive result from a fecal immunochemical test (FIT).
Methods: We used an established microsimulation model to simulate an average-risk United States population cohort that underwent annual FIT screening (from ages 50 to 75 years), with follow-up colonoscopy examinations for individuals with positive results (cutoff, 20 μg/g) at different time points in the following 12 months. Main evaluated outcomes were CRC incidence and mortality; additional outcomes were total life-years lost and net costs of screening.
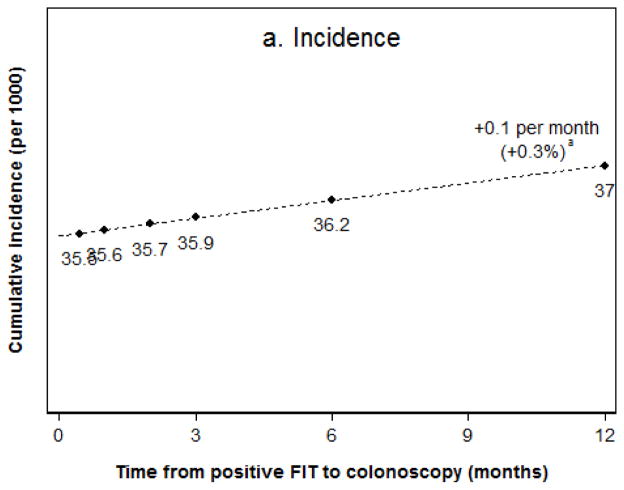
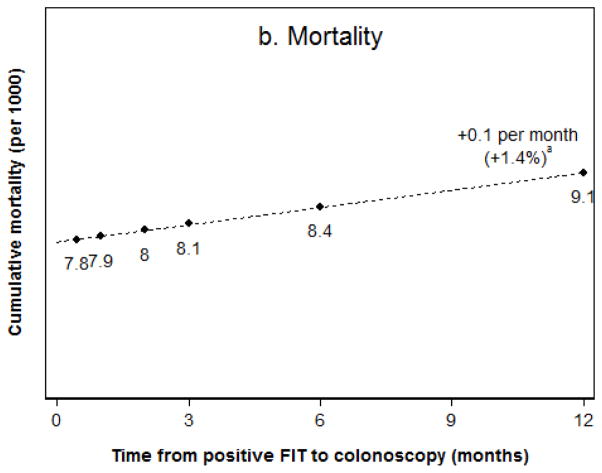
Results: For individuals who underwent diagnostic colonoscopy within 2 weeks of a positive result from an FIT, the estimated lifetime risk of CRC incidence was 35.5/1000 persons, and mortality was 7.8/1000 persons. Every month added until colonoscopy was associated with a 0.1/1000 person increase in cancer incidence risk (an increase of 0.3%/month, compared with individuals who received colonoscopies within 2 weeks) and mortality risk (increase of 1.4%/month). Among individuals who received colonoscopy examinations 12 months after a positive result from an FIT, the incidence of CRC was 37.0/1000 persons (increase of 4%, compared with 2 weeks), and mortality was 9.1/1000 persons (increase of 16%). Total years of life gained for the entire screening cohort decreased from an estimated 93.7/1000 persons with an almost immediate follow-up colonoscopy (cost savings of $208 per patient, compared with no colonoscopy) to 84.8/1000 persons with follow-up colonoscopies at 12 months (decrease of 9%; cost savings of $100/patient, compared with no colonoscopy).
Conclusions: By using a microsimulation model of an average-risk United States screening cohort, we estimated that delays of up to 12 months after a positive result from an FIT can produce proportional losses of up to nearly 10% in overall screening benefits. These findings indicate the importance of timely follow-up colonoscopy examinations of patients with positive results from FITs.
Keywords: Colorectal Neoplasms; Occult Blood; Screening and Early Detection; Time Factors.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. Epub 2014/01/09. - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MH, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996;348(9040):1472–7. - PubMed
-
- Kronborg O, Fenger C, Olsen J, et al. Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet. 1996;348(9040):1467–71. - PubMed
-
- Mandel JS, Church TR, Ederer F, et al. Colorectal cancer mortality: effectiveness of biennial screening for fecal occult blood. J Natl Cancer Inst. 1999;91(5):434–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
