

Early Impact of the Affordable Care Act on Uptake of Long-acting Reversible Contraceptive Methods
- PMID: 27213549
- PMCID: PMC4982821
- DOI: 10.1097/MLR.0000000000000551
Early Impact of the Affordable Care Act on Uptake of Long-acting Reversible Contraceptive Methods
Abstract
Background: The Affordable Care Act (ACA) required most private insurance plans to cover contraceptive services without patient cost-sharing as of January 2013 for most plans. Whether the ACA's mandate has impacted long-acting reversible contraceptives (LARC) use is unknown.
Objective: The aim of this article is to assess trends in LARC cost-sharing and uptake before and one year after implementation of the ACA's contraceptive mandate.
Design: A retrospective cohort study using Truven Health MarketScan claims data from January 2010 to December 2013.
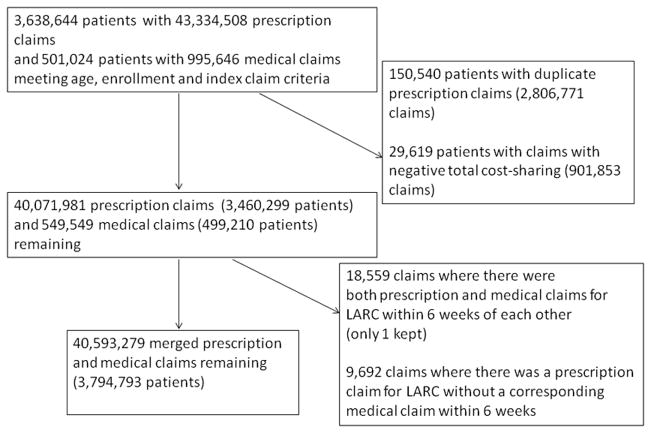
Subjects: Women aged 18-45 years with continuous insurance coverage with claims for oral contraceptive pills, patches, rings, injections, or LARC during 2010-2013 (N=3,794,793).
Measures: Descriptive statistics were used to assess trends in LARC cost-sharing and uptake from 2010 through 2013. Interrupted time series models were used to assess the association of time, ACA, and time after the ACA on LARC cost-sharing and initiation rates, adjusting for patient and plan characteristics.
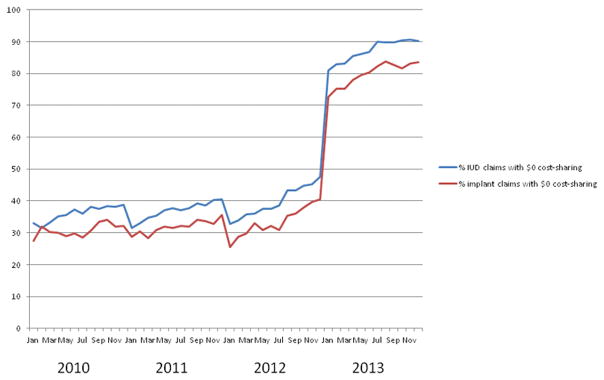
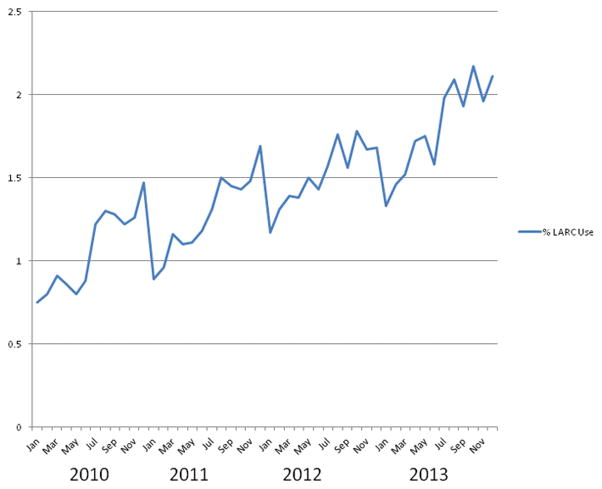
Results: The proportion of claims with $0 cost-sharing for intrauterine devices and implants, respectively, rose from 36.6% and 9.3% in 2010 to 87.6% and 80.5% in 2013. The ACA was associated with a significant increase in these proportions and in their rate of increase (level and slope change both P<0.001). LARC uptake increased over time with no significant change in level of LARC use after ACA implementation in January 2013 (P=0.44) and a slightly slower rate of growth post-ACA than previously reported (β coefficient for trend, -0.004; P<0.001).
Conclusions: The ACA has significantly decreased LARC cost-sharing, but during its first year had not yet increased LARC initiation rates.
Conflict of interest statement
Figures
Similar articles
-
Long-Acting Reversible Contraceptive Uptake before and after the Affordable Care Act Contraceptive Mandate in Women Undergoing First Trimester Surgical Abortion.Womens Health Issues. 2018 Jul-Aug;28(4):301-305. doi: 10.1016/j.whi.2018.04.007. Epub 2018 May 28. Womens Health Issues. 2018. PMID: 29853173
-
The Impact of the Affordable Care Act on Contraceptive Use and Costs among Privately Insured Women.Womens Health Issues. 2018 May-Jun;28(3):219-223. doi: 10.1016/j.whi.2018.01.005. Epub 2018 Mar 13. Womens Health Issues. 2018. PMID: 29544988
-
The impact of out-of-pocket costs on the use of intrauterine contraception among women with employer-sponsored insurance.Med Care. 2013 Nov;51(11):959-63. doi: 10.1097/MLR.0b013e3182a97b5d. Med Care. 2013. PMID: 24036995 Free PMC article.
-
Contraceptive Coverage and the Affordable Care Act.Obstet Gynecol Clin North Am. 2015 Dec;42(4):605-17. doi: 10.1016/j.ogc.2015.07.001. Epub 2015 Sep 16. Obstet Gynecol Clin North Am. 2015. PMID: 26598303 Free PMC article. Review.
-
Eliminating health disparities in unintended pregnancy with long-acting reversible contraception (LARC).Am J Obstet Gynecol. 2016 Jun;214(6):681-8. doi: 10.1016/j.ajog.2016.02.017. Epub 2016 Feb 12. Am J Obstet Gynecol. 2016. PMID: 26875950 Free PMC article. Review.
Cited by
-
Examining public knowledge and preferences for adult preventive services coverage.PLoS One. 2017 Dec 20;12(12):e0189661. doi: 10.1371/journal.pone.0189661. eCollection 2017. PLoS One. 2017. PMID: 29261757 Free PMC article.
-
Effects of the Affordable Care Act on Contraception, Pregnancy, and Pregnancy Termination Rates.Obstet Gynecol. 2025 Feb 1;145(2):196-203. doi: 10.1097/AOG.0000000000005796. Epub 2024 Nov 14. Obstet Gynecol. 2025. PMID: 39823363 Free PMC article.
-
Cost-sharing and adherence, clinical outcomes, health care utilization, and costs: A systematic literature review.J Manag Care Spec Pharm. 2023 Jan;29(1):4-16. doi: 10.18553/jmcp.2022.21270. Epub 2022 Apr 7. J Manag Care Spec Pharm. 2023. PMID: 35389285 Free PMC article.
-
Prescription Contraceptive Sales Following the Affordable Care Act.Matern Child Health J. 2019 May;23(5):657-666. doi: 10.1007/s10995-018-2680-1. Matern Child Health J. 2019. PMID: 30600517
-
The Affordable Care Act contraception mandate & unintended pregnancy in women of reproductive age: An analysis of the National Survey of Family Growth, 2008-2010 v. 2013-2015.Contraception. 2020 Jan;101(1):34-39. doi: 10.1016/j.contraception.2019.09.003. Epub 2019 Oct 23. Contraception. 2020. PMID: 31655071 Free PMC article.
References
-
- Brown SS, Eisenberg L. Unintended pregnancy and the well-being of children and families. JAMA. 1995 Nov 1;274(17):1332. - PubMed
-
- Sonfield A, Kost K. Public Costs from Unintended Pregnancies and the Role of Public Insurance Programs in Paying for Pregnancy-Related Care: National and State Estimates for 2010. New York: Guttmacher Institute; 2015.
-
- Committee On Preventive Services For Women IoM. Clinical Preventive Services for Women: Closing the Gaps. Washington, DC: National Academies Press; 2011.
-
- Department of HHS. [Accessed March 18, 2013];News Release: Affordable Care Act Ensures Women Receive Preventive Services at No Additional Cost. 2011 http://www.hhs.gov/news/press/2011pres/08/20110801b.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
