

Simultaneous urodynamic and anorectal manometry studies in children: insights into the relationship between the lower gastrointestinal and lower urinary tracts
- PMID: 27214097
- PMCID: PMC4880423
- DOI: 10.1111/nmo.12794
Simultaneous urodynamic and anorectal manometry studies in children: insights into the relationship between the lower gastrointestinal and lower urinary tracts
Abstract
Background: Children with urinary incontinence (UI) have associated functional constipation (FC) and fecal incontinence (FI). The physiology between lower urinary tract (LUT) and anorectum in children has not been elucidated.
Aims: Observe the effect of rectal distention (RD) on LUT function, and bladder filling and voiding on anorectal function.
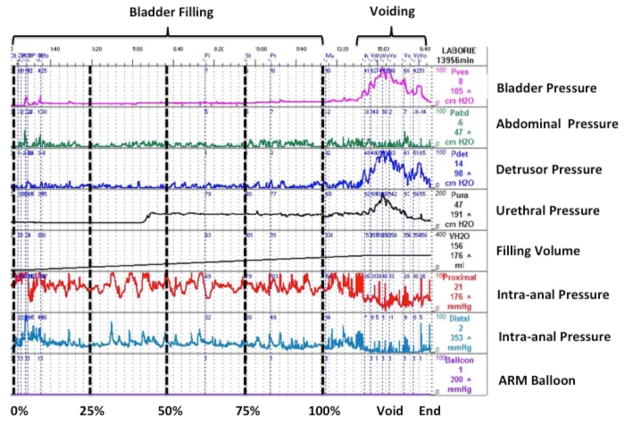
Methods: Children with voiding dysfunction referred to Boston Children's Hospital were prospectively enrolled in combined urodynamic (UDS) and anorectal manometry (ARM). Anorectal and urodynamic parameters were simultaneously measured. Patients underwent two micturition cycles, first with rectal balloon deflated and second with it inflated (RD). Lower urinary tract and anorectal parameters were compared between cycles.
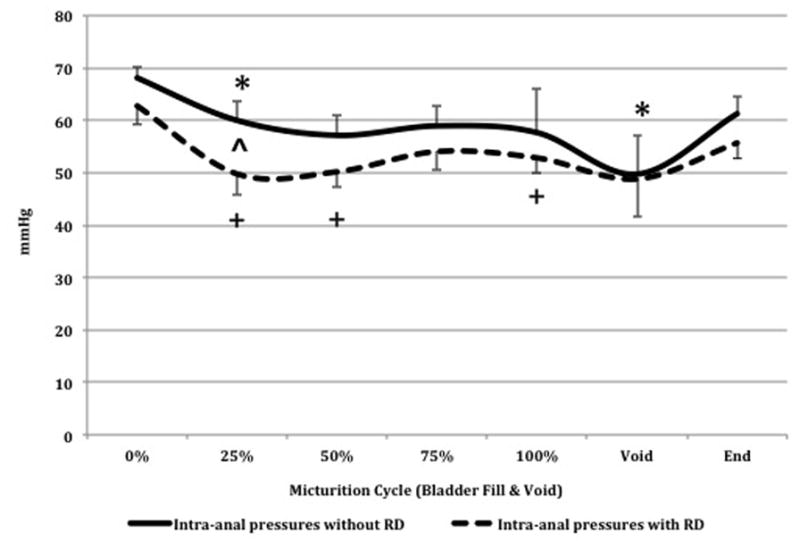
Key results: Ten children (seven UI, four recurrent UTIs, nine FC ± FI) were enrolled. Postvoid residual (PVR) increased (p = 0.02) with RD. No differences were observed in percent of bladder filling to expected bladder capacity, sensation, and bladder compliance with and without RD. Bladder and abdominal pressures increased at voiding with RD (p < 0.05). Intra-anal pressures decreased at voiding (p < 0.05), at 25% (p = 0.03) and 50% (p = 0.06) of total volume of bladder filling.
Conclusions & inferences: The PVR volume increased with RD. Stool in the rectum does not alter filling cystometric capacity but decreases the bladder's ability to empty predisposing patients with fecal retention to UI and UTIs. Bladder and abdominal pressures increased during voiding, demonstrating a physiological correlate of voiding dysfunction. Intra-anal pressures decreased during bladder filling and voiding. This is the first time intra-anal relaxation during bladder filling and voiding has been described.
Keywords: anorectal manometry; bowel and bladder dysfunction; children; constipation; fecal incontinence; urodynamics; voiding dysfunction.
© 2016 John Wiley & Sons Ltd.
Conflict of interest statement
Conflict of interest: None
Potential competing interests: None
Figures



Similar articles
-
Anorectal manometry and urodynamics in children with spina bifida: can we predict the colonic dysmotility from bladder dysfunction?BMC Urol. 2024 Dec 19;24(1):269. doi: 10.1186/s12894-024-01671-w. BMC Urol. 2024. PMID: 39702239 Free PMC article. Clinical Trial.
-
Videomanometry of the pelvic organs: a comparison of the normal lower urinary and gastrointestinal tracts.Int J Urol. 2006 Jan;13(1):29-35. doi: 10.1111/j.1442-2042.2006.01224.x. Int J Urol. 2006. PMID: 16448429
-
The influence of bladder filling on anorectal function.Colorectal Dis. 2003 May;5(3):251-5. doi: 10.1046/j.1463-1318.2003.00431.x. Colorectal Dis. 2003. PMID: 12780887
-
[Recommendations for the urodynamic examination in the investigation of non-neurological female urinary incontinence].Prog Urol. 2007 Nov;17(6 Suppl 2):1264-84. Prog Urol. 2007. PMID: 18214138 Review. French.
-
Urodynamic assessment of voiding dysfunction and dysfunctional voiding in girls and women.Int Urogynecol J Pelvic Floor Dysfunct. 2000;11(4):254-64. doi: 10.1007/s001920070035. Int Urogynecol J Pelvic Floor Dysfunct. 2000. PMID: 11005479 Review.
Cited by
-
Diagnosis and management of bladder bowel dysfunction in children with urinary tract infections: a position statement from the International Children's Continence Society.Pediatr Nephrol. 2018 Dec;33(12):2207-2219. doi: 10.1007/s00467-017-3799-9. Epub 2017 Oct 3. Pediatr Nephrol. 2018. PMID: 28975420
References
-
- Joinson C, Heron J, Butler U, von Gontard A. Psychological differences between children with and without soiling problems. Pediatrics. 2006;117(5):1575–84. - PubMed
-
- Joinson C, Heron J, von Gontard A. Psychological problems in children with daytime wetting. Pediatrics. 2006;118(5):1985–93. - PubMed
-
- Rajindrajith S, Devanarayana NM, Weerasooriya L, Hathagoda W, Benninga MA. Quality of life and somatic symptoms in children with constipation: a school-based study. J Pediatr. 2013;163(4):1069–72. e1. - PubMed
-
- Thibodeau BA, Metcalfe P, Koop P, Moore K. Urinary incontinence and quality of life in children. J Pediatr Urol. 2013;9(1):78–83. - PubMed
-
- van Dijk M, Benninga MA, Grootenhuis MA, Last BF. Prevalence and associated clinical characteristics of behavior problems in constipated children. Pediatrics. 2010;125(2):e309–17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
