

Optimizing safety and accuracy of prostate biopsy
- PMID: 27214580
- PMCID: PMC5011431
- DOI: 10.1097/MOU.0000000000000310
Optimizing safety and accuracy of prostate biopsy
Abstract
Purpose of review: The objective of this article is to examine the safety of prostate biopsy and discuss the emerging role of MRI-ultrasound fusion technology in improving diagnostic accuracy.
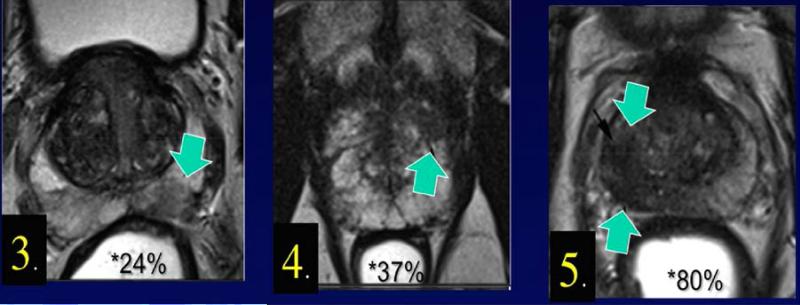
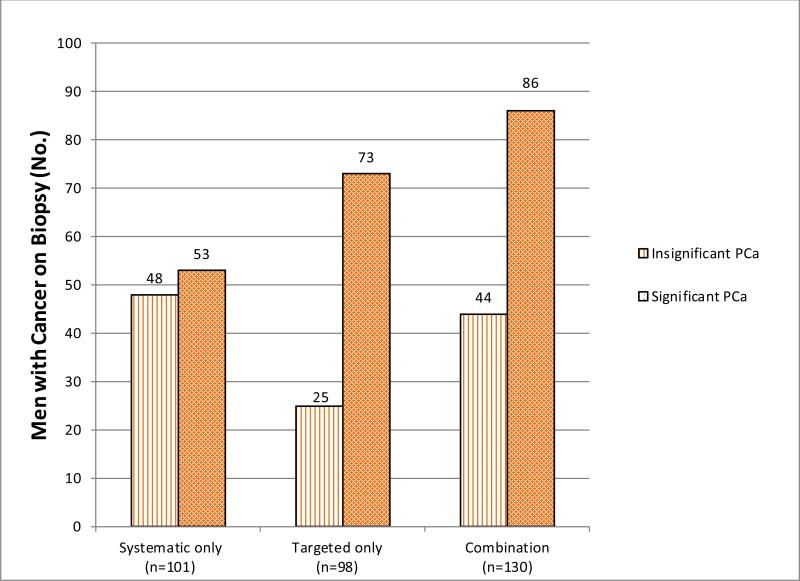
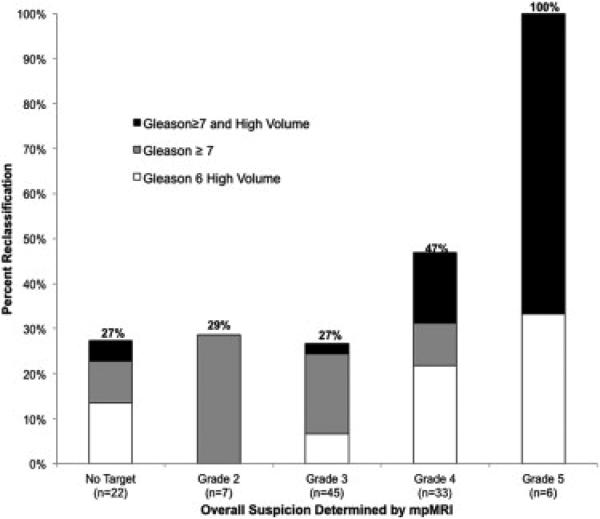
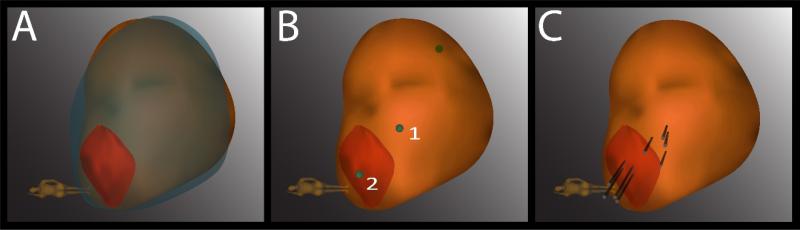
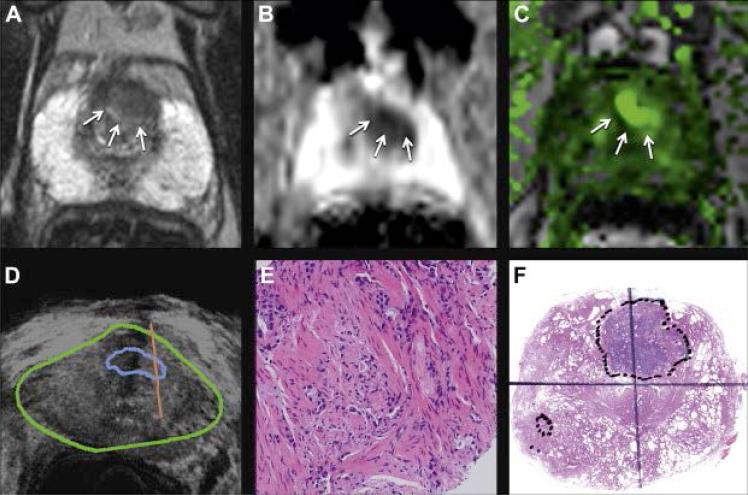
Recent findings: Men undergoing prostate biopsy frequently experience minor complications, including hematospermia, hematuria, and infection. Quinolone-resistant bacteria are a growing concern; thus, transperineal access or modification of antibiotic prophylaxis based on local antibiograms is now used to avoid infectious complications.Multiparametric MRI allows visualization of many prostate cancers, and by fusing MRI with real-time ultrasound, a biopsy needle can be directed by a urologist into suspicious regions of interest. Using this new method, detection of clinically significant prostate cancer has increased and the incidence of falsely negative biopsies has decreased.
Summary: Prostate biopsy is generally a safe procedure, and with attention to local patterns of antibiotic resistance, infectious complications can be minimized. MRI-ultrasound fusion has significantly improved the accuracy of prostate biopsy, allowing tracking and targeting not previously possible.
Figures
References
-
- Van Der Kwast T, Bubendorf L, Mazerolles C, et al. Guidelines on processing and reporting of prostate biopsies: The 2013 update of the pathology committee of the European Randomized Study of Screening for Prostate Cancer (ERSPC). Virchows Arch. 2013;463(3):367–77. - PubMed
-
- Lundstrom KJ, Drevin L, Carlsson S, et al. Nationwide population based study of infections after transrectal ultrasound guided prostate biopsy. J Urol. 2014;192:1116–22. - PubMed
-
- Cussans A, Somani BK, Basarab A, Dudderidge T. The role of targeted prophylactic antimicrobial therapy prior to transrectal ultrasound (TRUS) guided prostate biopsy in reducing infection rates: a systematic review. BJU Int [Internet] 2015 Available from: http://doi.wiley.com/10.1111/bju.13402. [This article discusses the importance of targeted prophylaxis in decreasing infection rates.] - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
