

Mechanisms linking electrical alternans and clinical ventricular arrhythmia in human heart failure
- PMID: 27215536
- PMCID: PMC4996715
- DOI: 10.1016/j.hrthm.2016.05.017
Mechanisms linking electrical alternans and clinical ventricular arrhythmia in human heart failure
Abstract
Background: Mechanisms of ventricular tachycardia (VT) and ventricular fibrillation (VF) in patients with heart failure (HF) are undefined.
Objective: The purpose of this study was to elucidate VT/VF mechanisms in HF by using a computational-clinical approach.
Methods: In 53 patients with HF and 18 control patients, we established the relationship between low-amplitude action potential voltage alternans (APV-ALT) during ventricular pacing at near-resting heart rates and VT/VF on long-term follow-up. Mechanisms underlying the transition of APV-ALT to VT/VF, which cannot be ascertained in patients, were dissected with multiscale human ventricular models based on human electrophysiological and magnetic resonance imaging data (control and HF).
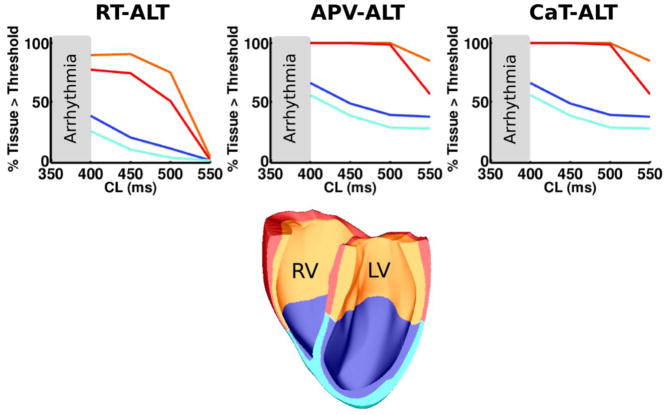
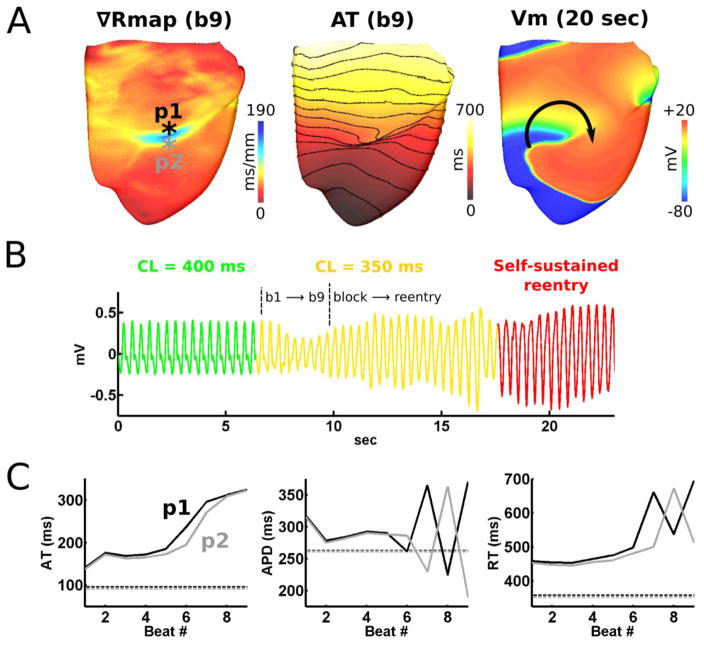
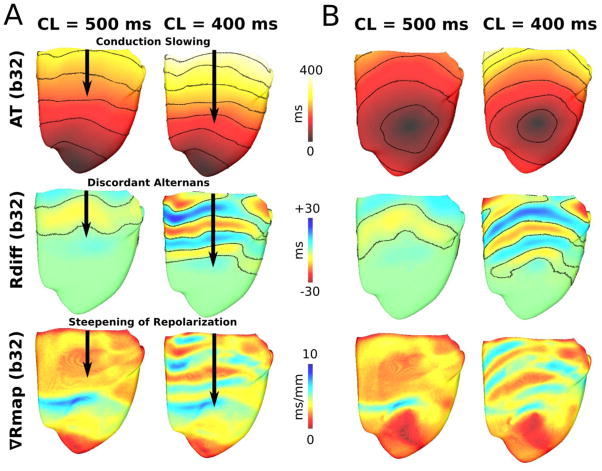
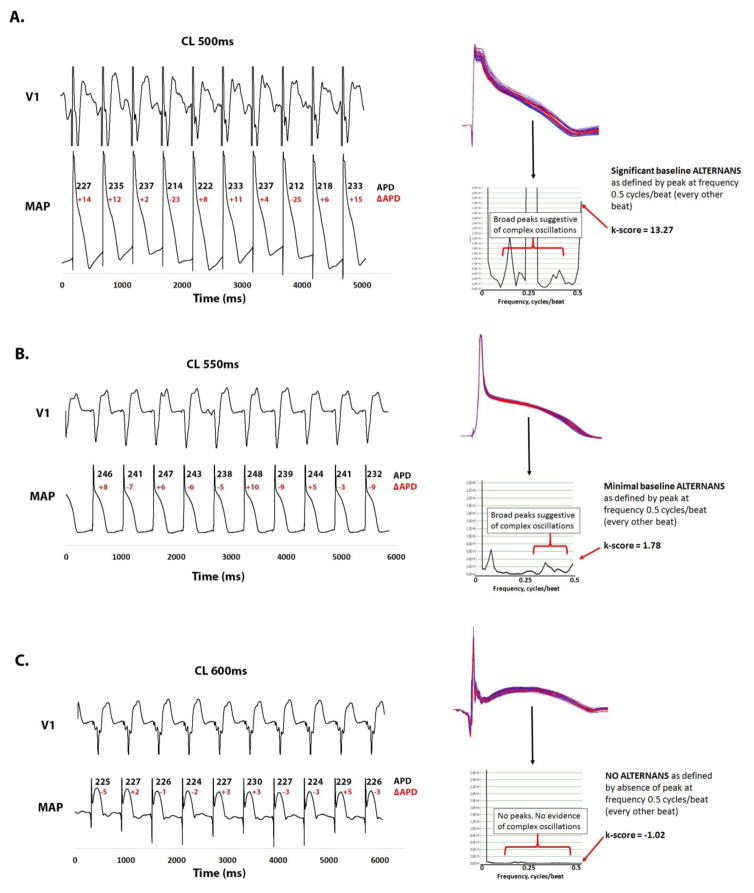
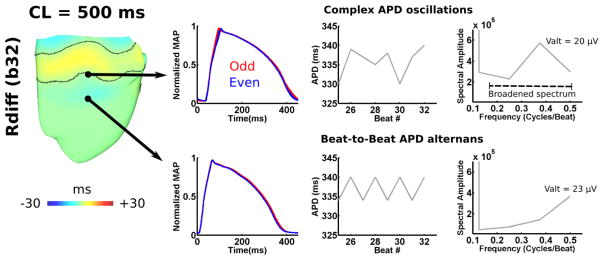
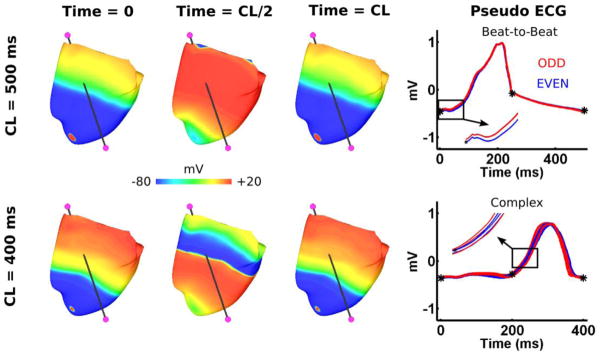
Results: For patients with APV-ALT k-score >1.7, complex action potential duration (APD) oscillations (≥2.3% of mean APD), rather than APD alternans, most accurately predicted VT/VF during long-term follow-up (+82%; -90% predictive values). In the failing human ventricular models, abnormal sarcoplasmic reticulum (SR) calcium handling caused APV-ALT (>1 mV) during pacing with a cycle length of 550 ms, which transitioned into large magnitude (>100 ms) discordant repolarization time alternans (RT-ALT) at faster rates. This initiated VT/VF (cycle length <400 ms) by steepening apicobasal repolarization (189 ms/mm) until unidirectional conduction block and reentry. Complex APD oscillations resulted from nonstationary discordant RT-ALT. Restoring SR calcium to control levels was antiarrhythmic by terminating electrical alternans.
Conclusion: APV-ALT and complex APD oscillations at near-resting heart rates in patients with HF are linked to arrhythmogenic discordant RT-ALT. This may enable novel physiologically tailored, bioengineered indices to improve VT/VF risk stratification, where SR calcium handling and spatial apicobasal repolarization are potential therapeutic targets.
Keywords: Alternans; Arrhythmia; Computational modeling; Heart failure; Simulation.
Copyright © 2016 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Heart failure enhances susceptibility to arrhythmogenic cardiac alternans.Heart Rhythm. 2009 Feb;6(2):251-9. doi: 10.1016/j.hrthm.2008.11.008. Epub 2008 Nov 8. Heart Rhythm. 2009. PMID: 19187920 Free PMC article.
-
Rate-dependent action potential alternans in human heart failure implicates abnormal intracellular calcium handling.Heart Rhythm. 2010 Aug;7(8):1093-101. doi: 10.1016/j.hrthm.2010.04.008. Epub 2010 Apr 8. Heart Rhythm. 2010. PMID: 20382266 Free PMC article.
-
Action potential dynamics explain arrhythmic vulnerability in human heart failure: a clinical and modeling study implicating abnormal calcium handling.J Am Coll Cardiol. 2008 Nov 25;52(22):1782-92. doi: 10.1016/j.jacc.2008.08.037. J Am Coll Cardiol. 2008. PMID: 19022157 Free PMC article.
-
Developing a novel comprehensive framework for the investigation of cellular and whole heart electrophysiology in the in situ human heart: historical perspectives, current progress and future prospects.Prog Biophys Mol Biol. 2014 Aug;115(2-3):252-60. doi: 10.1016/j.pbiomolbio.2014.06.004. Epub 2014 Jun 24. Prog Biophys Mol Biol. 2014. PMID: 24972083 Review.
-
Review of the predictive value of the Langendorff heart model (Screenit system) in assessing the proarrhythmic potential of drugs.J Pharmacol Toxicol Methods. 2004 May-Jun;49(3):171-81. doi: 10.1016/j.vascn.2004.03.008. J Pharmacol Toxicol Methods. 2004. PMID: 15172013 Review.
Cited by
-
Model Systems for Addressing Mechanism of Arrhythmogenesis in Cardiac Repair.Curr Cardiol Rep. 2021 May 29;23(6):72. doi: 10.1007/s11886-021-01498-z. Curr Cardiol Rep. 2021. PMID: 34050853 Free PMC article. Review.
-
Personalized Imaging and Modeling Strategies for Arrhythmia Prevention and Therapy.Curr Opin Biomed Eng. 2018 Mar;5:21-28. doi: 10.1016/j.cobme.2017.11.007. Curr Opin Biomed Eng. 2018. PMID: 29546250 Free PMC article.
-
Modulation of Cardiac Alternans by Altered Sarcoplasmic Reticulum Calcium Release: A Simulation Study.Front Physiol. 2018 Sep 19;9:1306. doi: 10.3389/fphys.2018.01306. eCollection 2018. Front Physiol. 2018. PMID: 30283355 Free PMC article.
-
Computational Identification of Ventricular Arrhythmia Risk in Pediatric Myocarditis.Pediatr Cardiol. 2019 Apr;40(4):857-864. doi: 10.1007/s00246-019-02082-7. Epub 2019 Mar 6. Pediatr Cardiol. 2019. PMID: 30840104 Free PMC article.
-
Learning for Prevention of Sudden Cardiac Death.Circ Res. 2021 Jan 22;128(2):185-187. doi: 10.1161/CIRCRESAHA.120.318576. Epub 2021 Jan 21. Circ Res. 2021. PMID: 33476206 Free PMC article. No abstract available.
References
-
- Pastore JM, Girouard SD, Laurita KR, Akar FG, Rosenbaum DS. Mechanism linking T-wave alternans to the genesis of cardiac fibrillation. Circulation. 1999;99:1385–1394. - PubMed
-
- Watanabe MA, Fenton FH, Evans SJ, Hastings HM, Karma A. Mechanisms for discordant alternans. J Cardiovasc Electr. 2001;12:196–206. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
