

Five-year visual acuity outcomes and injection patterns in patients with pro-re-nata treatments for AMD, DME, RVO and myopic CNV
- PMID: 27215744
- PMCID: PMC5339568
- DOI: 10.1136/bjophthalmol-2016-308668
Five-year visual acuity outcomes and injection patterns in patients with pro-re-nata treatments for AMD, DME, RVO and myopic CNV
Abstract
Background: Anti vascular endothelial growth factor (VEGF) therapy is an established treatment for various retinal diseases. Long-term data on injection frequencies and visual acuity (VA), however, are still rare.
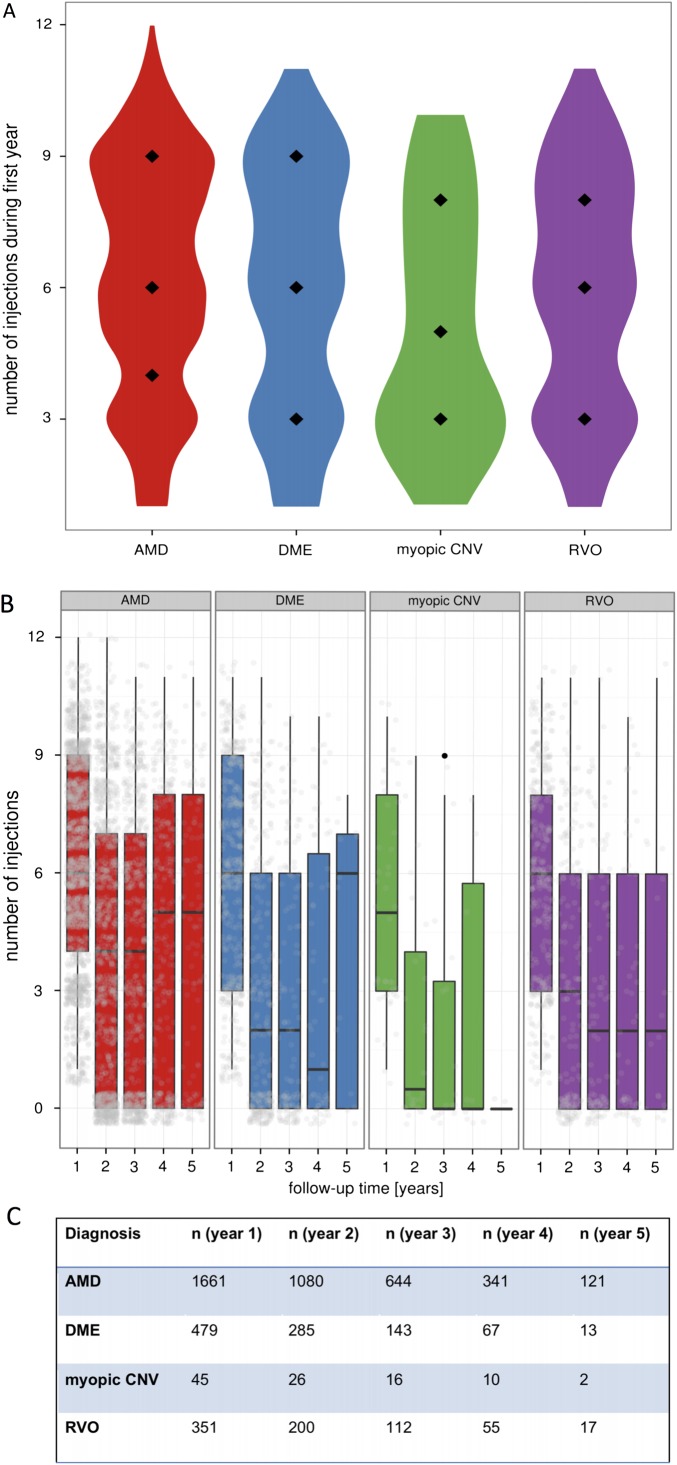
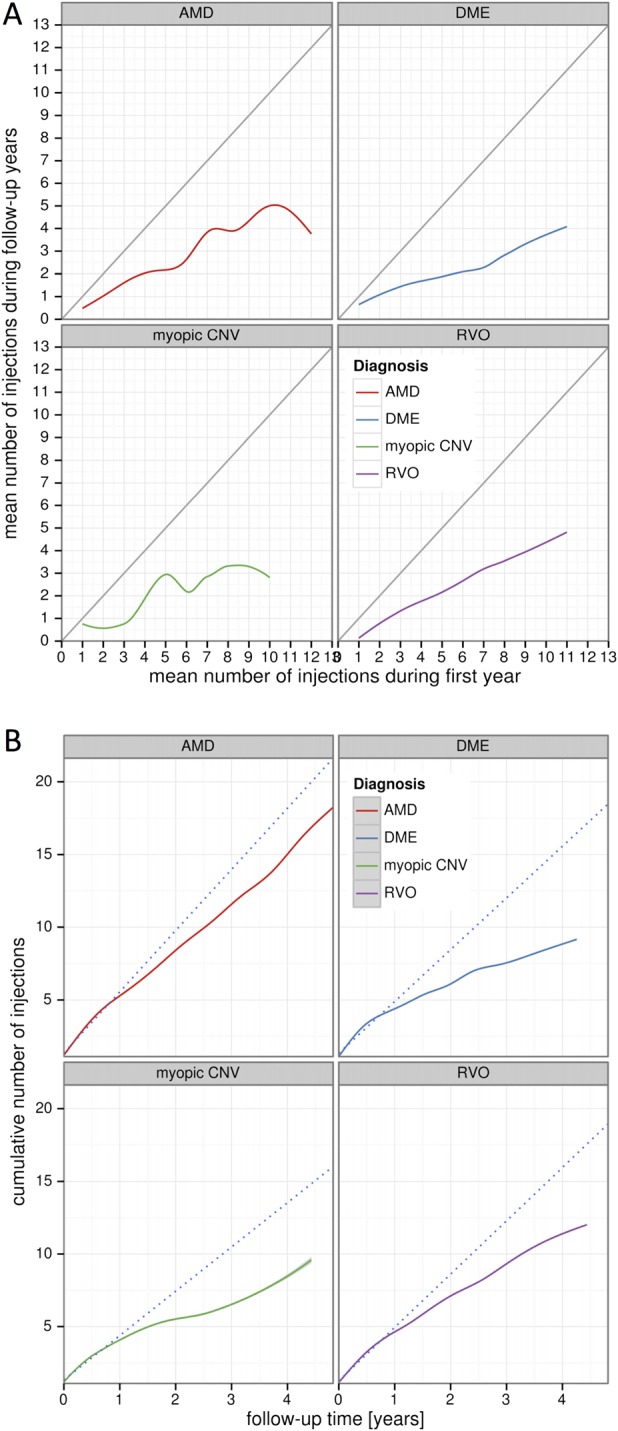
Methods: Five-year analysis of real-life VA developments and injection patterns from 2072 patients (2577 eyes; 33 187 injections) with chronically active disease undergoing pro-re-nata treatment for age-related macular degeneration (AMD), diabetic macular oedema (DME), retinal vein occlusion (RVO) and myopic choroidal neovascularisation (CNV).
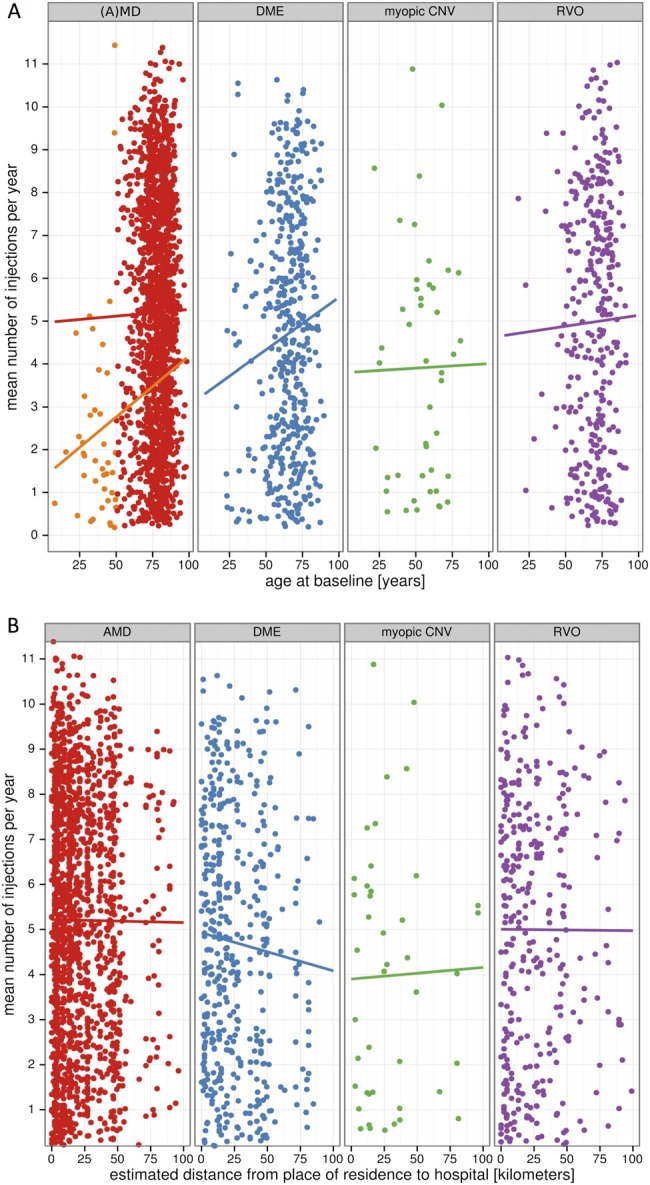
Results: Maximum mean VA gain in year 1 was+5.2 letters in AMD, +6.2 in DME, +10 in RVO and+7.2 in myopic CNV. Over 5 years, however, VA in patients with AMD declined. By year 5, 34% of patients with AMD had experienced VA loss of >15 letters, 56% had remained stable and 10% had gained >15 letters. Long-term VA developments in DME and RVO were more favourable with 81% of DME and 79% of patients with RVO gaining or maintaining vision at 5 years. In AMD, median injection frequency was six in year 1 and between four and five in consecutive years. In DME and RVO, median injection frequency was six in year 1 but lower compared with AMD in consecutive years. Injection frequency in DME was weakly associated with patient age (rs=0.1; p=0.03).
Conclusions: In AMD, the initial VA gain was not maintained long term despite higher injection numbers compared with DME, RVO and myopic CNV. The presented real-world data provide a peer-group-based estimate of VA developments and injection frequencies for counselling patients undergoing long-term anti-VEGF therapy.
Keywords: Angiogenesis; Macula; Neovascularisation; Retina.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: None declared.
Figures


References
-
- Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Optical coherence tomography findings after an intravitreal injection of bevacizumab (avastin) for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging 2005;36:331–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical