

The epidemiology of residual Plasmodium falciparum malaria transmission and infection burden in an African city with high coverage of multiple vector control measures
- PMID: 27216734
- PMCID: PMC4877954
- DOI: 10.1186/s12936-016-1340-4
The epidemiology of residual Plasmodium falciparum malaria transmission and infection burden in an African city with high coverage of multiple vector control measures
Abstract
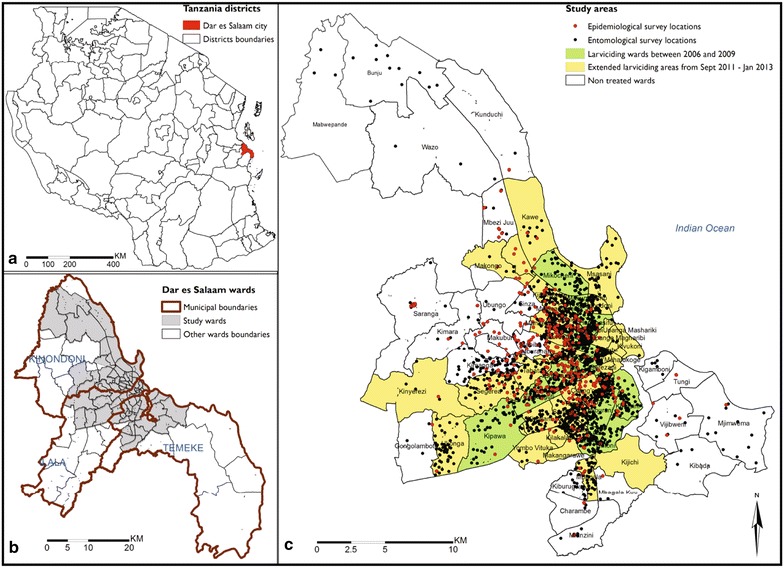
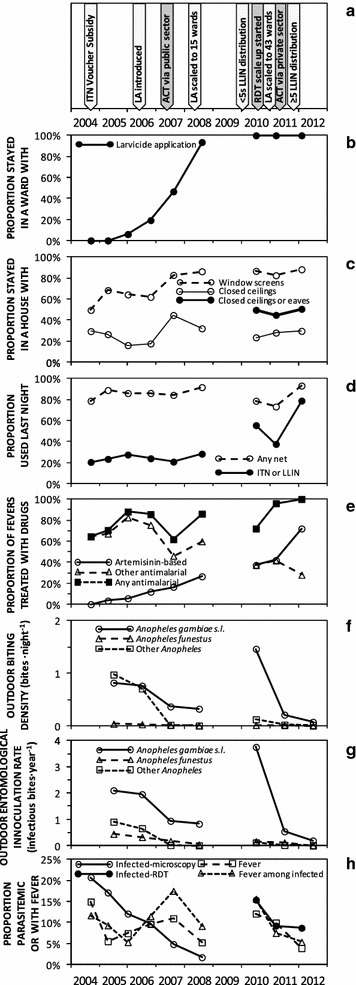
Background: In the Tanzanian city of Dar es Salaam, high coverage of long-lasting insecticidal nets (LLINs), larvicide application (LA) and mosquito-proofed housing, was complemented with improved access to artemisinin-based combination therapy and rapid diagnostic tests by the end of 2012.
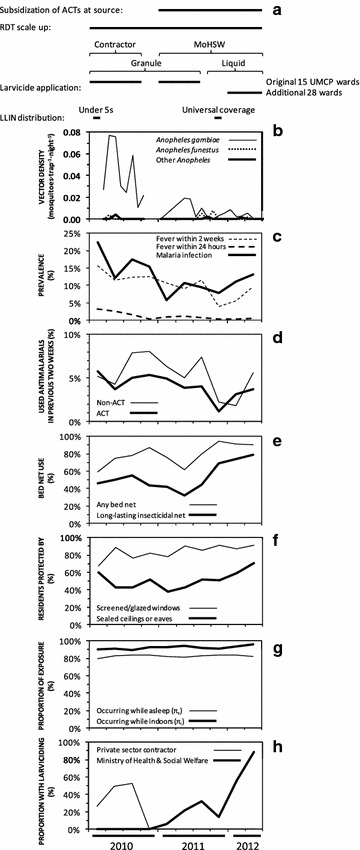
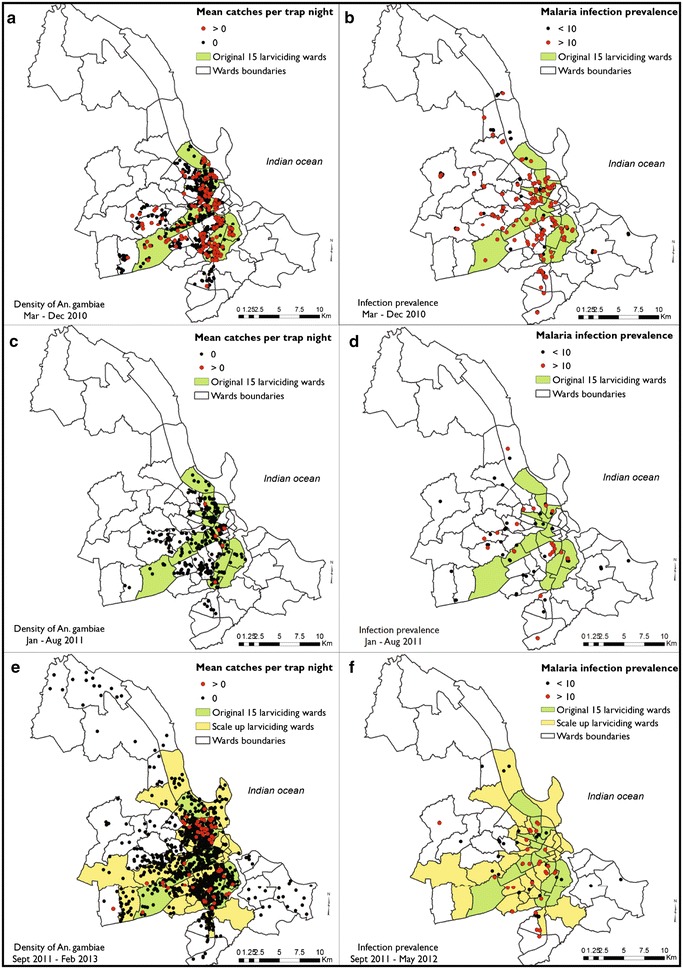
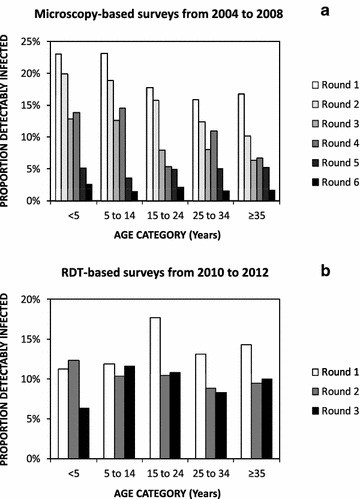
Methods: Three rounds of city-wide, cluster-sampled cross-sectional surveys of malaria parasite infection status, spanning 2010 to 2012, were complemented by two series of high-resolution, longitudinal surveys of vector density.
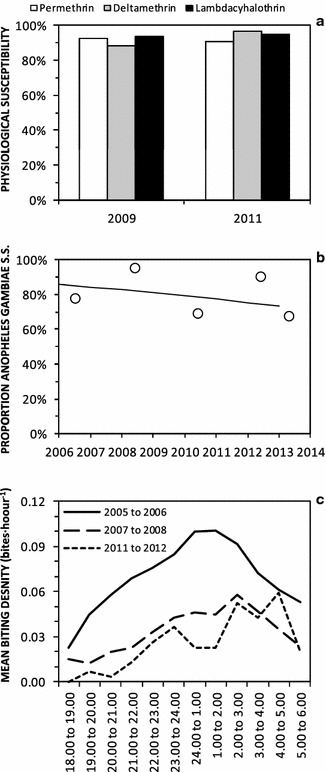
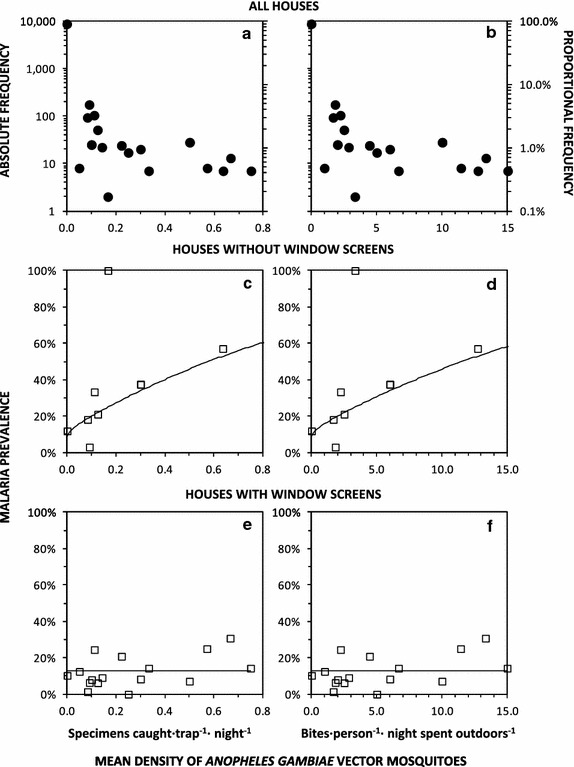
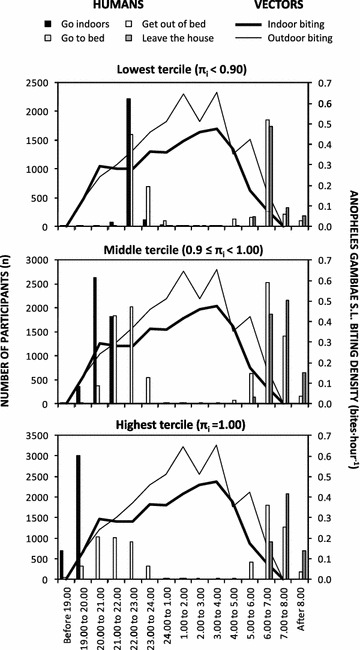
Results: Larvicide application using a granule formulation of Bacillus thuringiensis var. israelensis (Bti) had no effect upon either vector density (P = 0.820) or infection prevalence (P = 0.325) when managed by a private-sector contractor. Infection prevalence rebounded back to 13.8 % in 2010, compared with <2 % at the end of a previous Bti LA evaluation in 2008. Following transition to management by the Ministry of Health and Social Welfare (MoHSW), LA consistently reduced vector densities, first using the same Bti granule in early 2011 [odds ratio (OR) (95 % confidence interval (CI)) = 0.31 (0.14, 0.71), P = 0.0053] and then a pre-diluted aqueous suspension formulation from mid 2011 onwards [OR (95 % CI) = 0.15 (0.07, 0.30), P ≪ 0.000001]. While LA by MoHSW with the granule formulation was associated with reduced infection prevalence [OR (95 % CI) = 0.26 (0.12, 0.56), P = 0.00040], subsequent liquid suspension use, following a mass distribution to achieve universal coverage of LLINs that reduced vector density [OR (95 % CI) = 0.72 (0.51, 1.01), P = 0.057] and prevalence [OR (95 % CI) = 0.80 (0.69, 0.91), P = 0.0013], was not associated with further prevalence reduction (P = 0.836). Sleeping inside houses with complete window screens only reduced infection risk [OR (95 % CI) = 0.71 (0.62, 0.82), P = 0.0000036] if the evenings and mornings were also spent indoors. Furthermore, infection risk was only associated with local vector density [OR (95 % CI) = 6.99 (1.12, 43.7) at one vector mosquito per trap per night, P = 0.037] among the minority (14 %) of households lacking screening. Despite attenuation of malaria transmission and immunity, 88 % of infected residents experienced no recent fever, only 0.4 % of these afebrile cases had been treated for malaria, and prevalence remained high (9.9 %) at the end of the study.
Conclusions: While existing vector control interventions have dramatically attenuated malaria transmission in Dar es Salaam, further scale-up and additional measures to protect against mosquito bites outdoors are desirable. Accelerated elimination of chronic human infections persisting at high prevalence will require active, population-wide campaigns with curative drugs.
Keywords: Anopheles; Chronic infection; Housing; Larval source management; Long-lasting insecticidal net; Malaria; Mosquito; Plasmodium; Vector control; Window screening.
Figures
References
-
- Robert V, MacIntyre K, Keating J, Trape JF, Duchemin JB, Warren M, et al. Malaria transmission in urban sub-Saharan Africa. Am J Trop Med Hyg. 2003;68:169–176. - PubMed
-
- Keiser J, Utzinger J, Castro MC, Smith TA, Tanner M, Singer BH. Urbanization in sub-Saharan Africa and implications for malaria control. Am J Trop Med Hyg. 2004;71(Supplement 2):118–127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
