

Paediatric brainstem: A comprehensive review of pathologies on MR imaging
- PMID: 27216793
- PMCID: PMC4956624
- DOI: 10.1007/s13244-016-0496-3
Paediatric brainstem: A comprehensive review of pathologies on MR imaging
Abstract
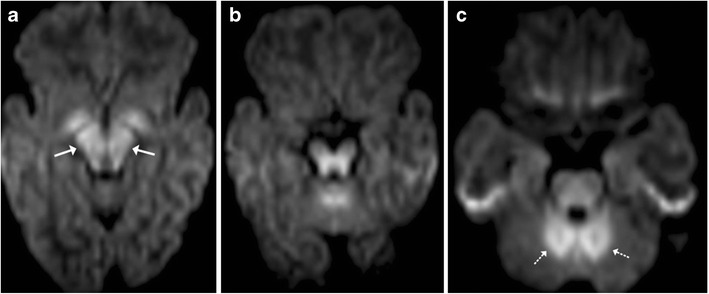
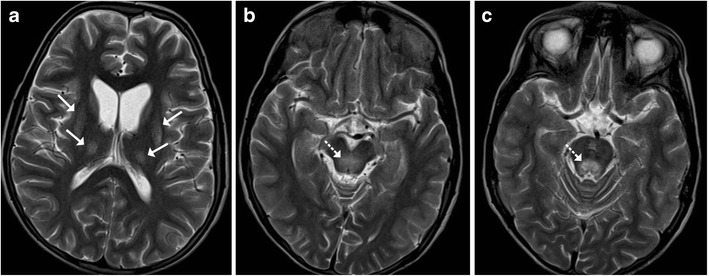
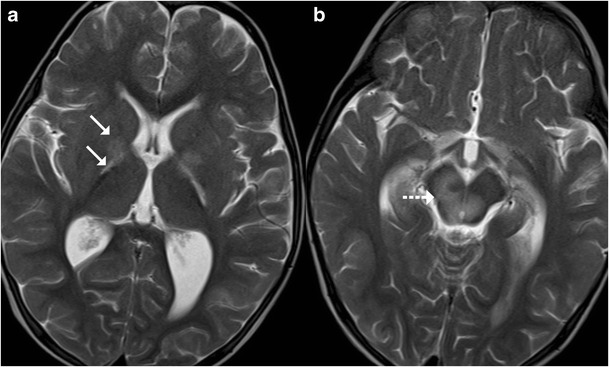
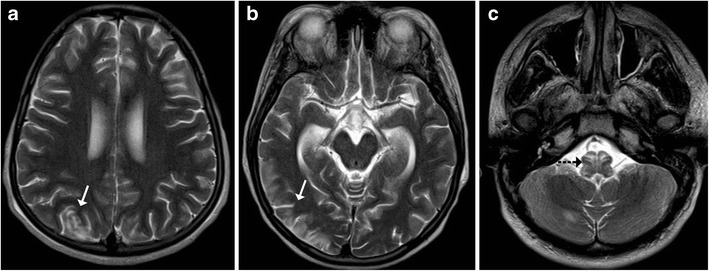
The brainstem is a midline structure formed by the midbrain, pons and medulla and is a home for various vital neurological centres of the human body. A diverse spectrum of disease entities can involve the brainstem, which includes infections, metabolic disorders, demyelination, vascular conditions, neurodegenerative disorders and tumours. Brainstem involvement can be primary or secondary, i.e., as part of systemic disorders. Due to the overlapping clinical presentation and symptomatology, imaging plays a decisive role in the detection, localisation and characterisation of brainstem pathologies. Magnetic resonance imaging (MRI) is the modality of choice and the use of advanced MR techniques such as diffusion-weighted imaging and spectroscopy can be especially helpful in providing a tenable diagnoses. This article is a compilation of the MR imaging manifestations of a spectrum of common and uncommon brainstem pathologies that can be encountered in the paediatric age group. Teaching Points • The paediatric brainstem can be afflicted by many pathologies that may overlap clinico-radiologically. • MRI is the best modality for the localisation and diagnosis of brainstem pathologies. • Diffusion-weighted imaging is useful in the diagnosis of vascular and metabolic disorders. • Occasionally, demyelination and neoplasms can be indistinguishable on imaging.
Keywords: Brainstem; Demyelination; Encephalitis; Glioma; MRI.
Figures

Similar articles
-
Magnetic resonance imaging of the brainstem in children, part 2: acquired pathology of the pediatric brainstem.Pediatr Radiol. 2021 Feb;51(2):189-204. doi: 10.1007/s00247-020-04954-0. Epub 2021 Jan 19. Pediatr Radiol. 2021. PMID: 33464360 Review.
-
Magnetic resonance imaging of the brainstem in children, part 1: imaging techniques, embryology, anatomy and review of congenital conditions.Pediatr Radiol. 2021 Feb;51(2):172-188. doi: 10.1007/s00247-020-04953-1. Epub 2021 Jan 26. Pediatr Radiol. 2021. PMID: 33496830 Review.
-
Measurement of brainstem diameter in small-breed dogs using magnetic resonance imaging.Front Vet Sci. 2023 Jul 13;10:1183412. doi: 10.3389/fvets.2023.1183412. eCollection 2023. Front Vet Sci. 2023. PMID: 37519998 Free PMC article.
-
A prospective study of magnetic resonance imaging patterns of central nervous system infections in pediatric age group and young adults and their clinico-biochemical correlation.J Pediatr Neurosci. 2016 Jan-Mar;11(1):46-51. doi: 10.4103/1817-1745.181244. J Pediatr Neurosci. 2016. PMID: 27195033 Free PMC article.
-
DTI fiber tracking to differentiate demyelinating diseases from diffuse brain stem glioma.Neuroimage. 2010 Aug 1;52(1):217-23. doi: 10.1016/j.neuroimage.2010.03.079. Epub 2010 Apr 2. Neuroimage. 2010. PMID: 20363335
Cited by
-
High mortality rates and long-term complications in children with infectious brainstem encephalitis: A study of sixteen cases.PLoS One. 2025 Feb 4;20(2):e0318818. doi: 10.1371/journal.pone.0318818. eCollection 2025. PLoS One. 2025. PMID: 39903731 Free PMC article.
-
Contemporary Management of Pediatric Brainstem Tumors.Adv Tech Stand Neurosurg. 2024;49:231-254. doi: 10.1007/978-3-031-42398-7_11. Adv Tech Stand Neurosurg. 2024. PMID: 38700687 Review.
-
Feasibility of Measuring GABA Levels in the Upper Brainstem in Healthy Volunteers Using Edited MRS.Front Psychiatry. 2020 Aug 14;11:813. doi: 10.3389/fpsyt.2020.00813. eCollection 2020. Front Psychiatry. 2020. PMID: 32922319 Free PMC article.
-
Paediatric rhombencephalitis presenting with bradycardia: a good recovery despite cardiac involvement.BMJ Case Rep. 2021 Nov 9;14(11):e244189. doi: 10.1136/bcr-2021-244189. BMJ Case Rep. 2021. PMID: 34753718 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
