

Efficacy of Prophylactic Mesh in End-Colostomy Construction: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- PMID: 27216806
- PMCID: PMC5028399
- DOI: 10.1007/s00268-016-3576-0
Efficacy of Prophylactic Mesh in End-Colostomy Construction: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Abstract
Background: Parastomal hernia is a very common complication after colostomy, especially end-colostomy. It is unclear whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer. A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction.
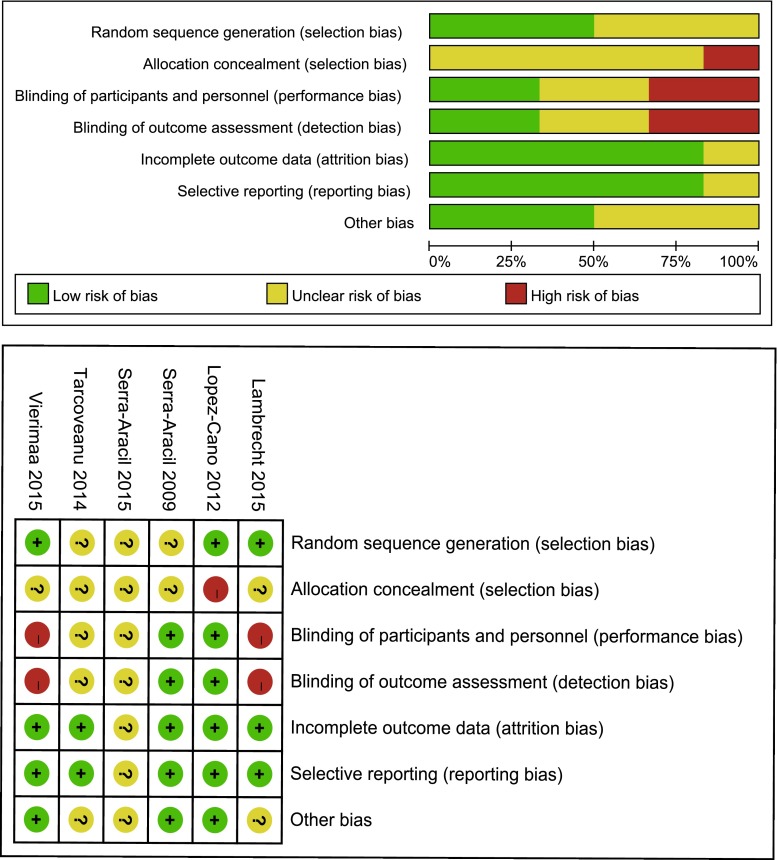
Methods: PubMed, Embase, and the Cochrane Library were searched, covering records entered from their inception to September 2015. Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included. The primary outcome was the incidence of parastomal hernia. Pooled risk ratios (RR) with 95 % confidence intervals (CI) were obtained using random effects models.
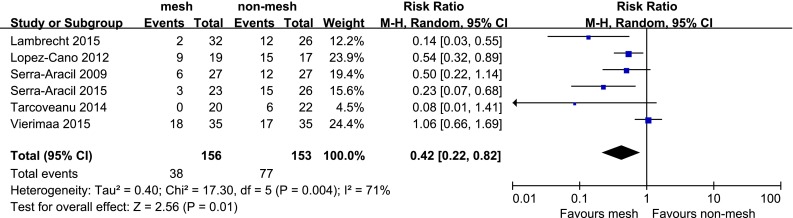
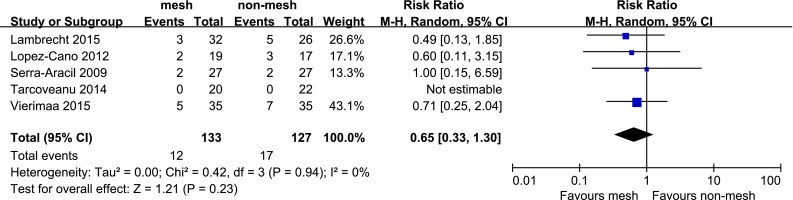
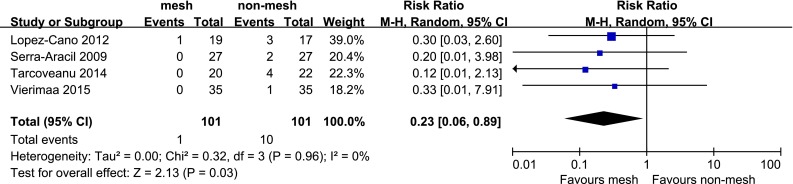
Results: Six RCTs containing 309 patients were included. Parastomal hernia occurred in 24.4 % (38 of 156) of patients with mesh and 50.3 % (77 of 153) of patients without mesh. Meta-analysis showed a lower incidence of parastomal hernia (RR, 0.42; 95 % CI 0.22-0.82) and reoperation related to parastomal hernia (RR, 0.23; 95 % CI 0.06-0.89) in patients with mesh. Stoma-related morbidity was similar between mesh group and non-mesh group (RR, 0.65; 95 % CI 0.33-1.30).
Conclusions: Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer, but not the rate of stoma-related morbidity. However, the results should be interpreted with caution because of the heterogeneity among the studies.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Hamada M, Tamura T, Sakamoto S, et al. Laparoscopic treatment of parastomal hernia using sugerbaker technique with parietex composite mesh. Surg Endosc Other Interv Tech. 2013;27:S389.
-
- Hotouras A, Thaha MA, Power N, et al. Preventing parastomal hernias: How critical is the trephine size? Colorectal Dis. 2011;13:45.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
