

Effects of CYP3A5 polymorphism on the pharmacokinetics of a once-daily modified-release tacrolimus formulation and acute kidney injury in hematopoietic stem cell transplantation
- PMID: 27217047
- PMCID: PMC4921119
- DOI: 10.1007/s00280-016-3060-4
Effects of CYP3A5 polymorphism on the pharmacokinetics of a once-daily modified-release tacrolimus formulation and acute kidney injury in hematopoietic stem cell transplantation
Abstract
Background: Tacrolimus is metabolized by cytochrome P450 (CYP) 3A4 and 3A5. We investigated the influence of CYP3A5 polymorphism and concurrent use of azole antifungal agents (AZ) on the pharmacokinetics of a once-daily modified-release tacrolimus formulation (Tac-QD) in patients after hematopoietic stem cell transplantation (HSCT).
Design and methods: Twenty-four patients receiving allogeneic HSCT were enrolled. Genotyping for CYP3A5*3 was done by a PCR-restriction fragment length polymorphism method. Trough blood concentrations (C0) of tacrolimus were measured by chemiluminescence magnetic microparticle immunoassay. Continuous infusion of tacrolimus was administered from the day before transplantation and was switched to Tac-QD after adequate oral intake.
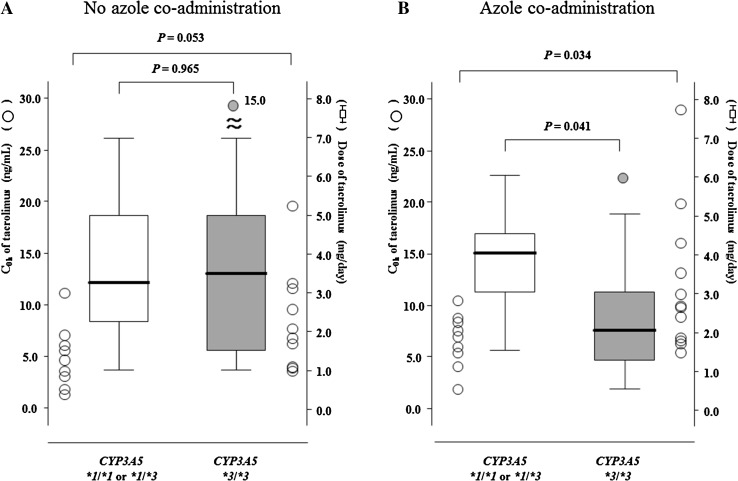
Results: Thirteen patients had a CYP3A5*3/*3 genotype, and 11 patients had a CYP3A5*1/*1 or *1/*3 genotype. No significant difference was observed in daily dosages and the C0 of tacrolimus between the two genotype groups without AZ. However, in patients who were co-administered AZ, the C0 values of tacrolimus were higher in patients with the CYP3A5*3/*3 allele than with the CYP3A5*1 allele (P = 0.034), although daily doses of Tac-QD in patients with CYP3A5*3/*3 were significantly lower than those with the CYP3A5*1 allele (P = 0.041). The cumulative incidence of acute kidney injury was higher in patients with the CYP3A5*3/*3 than with the CYP3A5*1 allele when AZ was co-administered. The decrement for daily dosage of Tac-QD was significantly greater in patients expressing the CYP3A5*3/*3 than the CYP3A5*1 allele.
Conclusions: CYP3A5 genotyping may be useful for safe and effective immunosuppressive therapy with Tac-QD in HSCT patients in whom the use of AZ is anticipated.
Keywords: Azole antifungal agent; CYP3A5 polymorphism; Hematopoietic stem cell transplantation; Once-daily tacrolimus formulation; Pharmacokinetics.
Figures


Similar articles
-
Comparison of pharmacokinetics and pharmacogenetics of once- and twice-daily tacrolimus in the early stage after renal transplantation.Transplantation. 2012 Nov 27;94(10):1013-9. doi: 10.1097/TP.0b013e31826bc400. Transplantation. 2012. PMID: 23073468
-
Combinational Effect of CYP3A5 and MDR-1 Polymorphisms on Tacrolimus Pharmacokinetics in Liver Transplant Patients.Exp Clin Transplant. 2015 Oct;13(5):441-8. Exp Clin Transplant. 2015. PMID: 26450467
-
CYP3A5*3 and ABCB1 61A>G Significantly Influence Dose-adjusted Trough Blood Tacrolimus Concentrations in the First Three Months Post-Kidney Transplantation.Basic Clin Pharmacol Toxicol. 2018 Sep;123(3):320-326. doi: 10.1111/bcpt.13016. Epub 2018 May 7. Basic Clin Pharmacol Toxicol. 2018. PMID: 29603629
-
[Innovative Personalized Medicine for Immunosuppressive Drugs Based on Novel Control Theory of Pharmacokinetics].Yakugaku Zasshi. 2024;144(12):1075-1080. doi: 10.1248/yakushi.24-00140. Yakugaku Zasshi. 2024. PMID: 39617470 Review. Japanese.
-
Effects of CYP3A4*22 polymorphism on trough concentration of tacrolimus in kidney transplantation: a systematic review and meta-analysis.Front Pharmacol. 2023 Jul 26;14:1201083. doi: 10.3389/fphar.2023.1201083. eCollection 2023. Front Pharmacol. 2023. PMID: 37564175 Free PMC article.
Cited by
-
Evaluation of genetic polymorphism of CYP3A5 in normal healthy participants from western India - A cross-sectional study.Indian J Pharmacol. 2022 Mar-Apr;54(2):97-101. doi: 10.4103/ijp.ijp_279_21. Indian J Pharmacol. 2022. PMID: 35546460 Free PMC article.
-
Polymorphisms in CYP3A5, CYP3A4, and ABCB1 genes: implications for calcineurin inhibitors therapy in hematopoietic cell transplantation recipients-a systematic review.Front Pharmacol. 2025 Jul 16;16:1569353. doi: 10.3389/fphar.2025.1569353. eCollection 2025. Front Pharmacol. 2025. PMID: 40740999 Free PMC article.
-
Impact of CYP3A5, POR, and CYP2C19 Polymorphisms on Trough Concentration to Dose Ratio of Tacrolimus in Allogeneic Hematopoietic Stem Cell Transplantation.Int J Mol Sci. 2019 May 15;20(10):2413. doi: 10.3390/ijms20102413. Int J Mol Sci. 2019. PMID: 31096684 Free PMC article.
-
Effects of clotrimazole on tacrolimus pharmacokinetics in patients with heart transplants with different CYP3A5 genotypes.Eur J Clin Pharmacol. 2019 Jan;75(1):67-75. doi: 10.1007/s00228-018-2558-6. Epub 2018 Sep 25. Eur J Clin Pharmacol. 2019. PMID: 30251062
-
[The effect of CYP3A5 gene polymorphism on tacrolimus concentration and adverse events in patients undergoing allogeneic hematopoietic stem cell transplantation].Zhonghua Xue Ye Xue Za Zhi. 2021 Oct 14;42(10):828-833. doi: 10.3760/cma.j.issn.0253-2727.2021.10.006. Zhonghua Xue Ye Xue Za Zhi. 2021. PMID: 34788922 Free PMC article. Chinese.
References
-
- Doesch AO, Mueller S, Konstandin M, et al. Increased adherence after switch from twice daily calcineurin inhibitor based treatment to once daily modified released tacrolimus in heart transplantation: a pre-experimental study. Transplant Proc. 2010;42:4238–4242. doi: 10.1016/j.transproceed.2010.09.074. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
