

Inpatient Mortality Among Solid Organ Transplant Recipients Hospitalized for Sepsis and Severe Sepsis
- PMID: 27217215
- PMCID: PMC4928388
- DOI: 10.1093/cid/ciw295
Inpatient Mortality Among Solid Organ Transplant Recipients Hospitalized for Sepsis and Severe Sepsis
Abstract
Background: Solid organ transplant (SOT) recipients are at elevated risk of sepsis. The impact of SOT on outcomes following sepsis is unclear.
Methods: We performed a retrospective cohort study using data from University HealthSystem Consortium, a consortium of academic medical center affiliates. We examined the association between SOT and mortality among patients hospitalized with severe sepsis or explicitly coded sepsis in 2012-2014. We used International Classification of Diseases, Ninth Revision (ICD-9) codes to identify severe sepsis, explicitly coded sepsis, and SOT (kidney, liver, heart, lung, pancreas, or intestine transplants). We fit random-intercept logistic regression models to account for clustering by hospital.
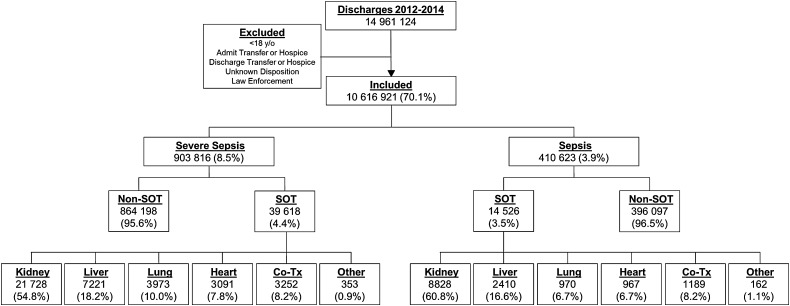
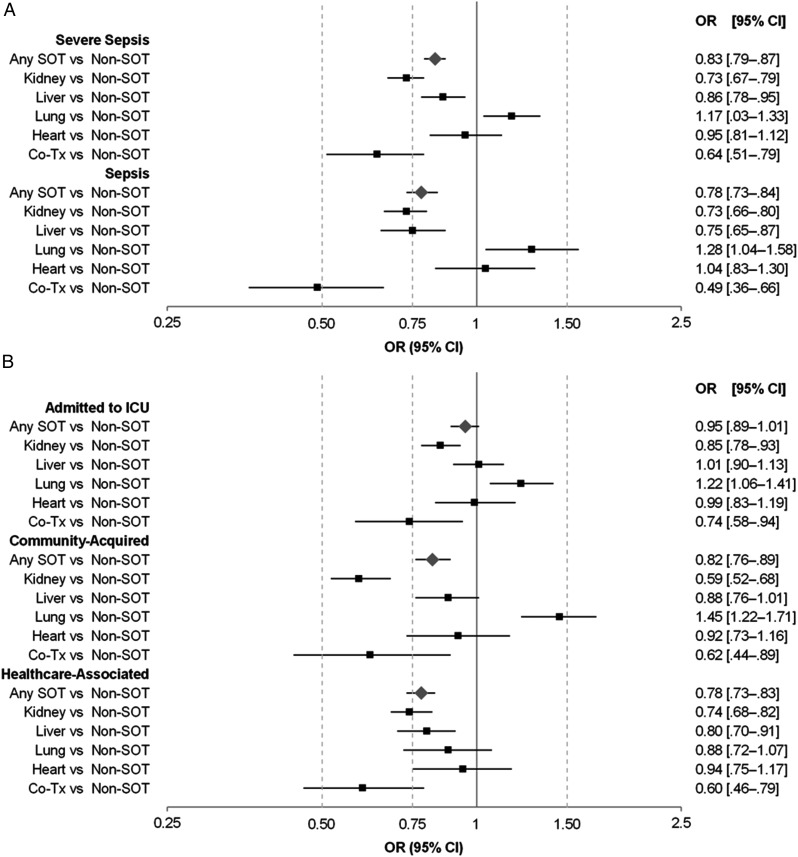
Results: There were 903 816 severe sepsis hospitalizations (39 618 [4.4%] with SOT) and 410 623 sepsis hospitalizations (14 526 [3.9%] with SOT) in 250 hospitals. SOT recipients were younger and more likely to be insured by Medicare than those without SOT. Among hospitalizations for severe sepsis and sepsis, in-hospital mortality was lower among those with vs those without SOT (5.5% vs 9.4% for severe sepsis; 8.7% vs 12.7% for sepsis). After adjustment, the odds ratio for mortality comparing SOT patients vs non-SOT was 0.83 (95% confidence interval [CI], .79-.87) for severe sepsis and 0.78 (95% CI, .73-.84) for sepsis. Compared to non-SOT patients, kidney, liver, and co-transplant (kidney-pancreas/kidney-liver) recipients demonstrated lower mortality. No association was present for heart transplant, and lung transplant was associated with higher mortality.
Conclusions: Among patients hospitalized for severe sepsis or sepsis, those with SOT had lower inpatient mortality than those without SOT. Identifying the specific strategies employed for populations with improved mortality could inform best practices for sepsis among SOT and non-SOT populations.
Keywords: critical care; infection; outcomes; sepsis; transplant.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- United Network for Organ Sharing. Donation and transplantation data. Available at: http://www.unos.org/donation/index.php?topic=data Accessed 16 May 2015.
-
- Wolfe RA, Ashby VB, Milford EL et al. . Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999; 341:1725–30. - PubMed
-
- Wolfe RA, McCullough KP, Schaubel DE et al. . Calculating life years from transplant (LYFT): methods for kidney and kidney-pancreas candidates. Am J Transplant 2008; 8:997–1011. - PubMed
-
- Abbott KC, Oliver JD 3rd, Hypolite I et al. . Hospitalizations for bacterial septicemia after renal transplantation in the United States. Am J Nephrol 2001; 21:120–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
