

Randomized, Prospective Evaluation Comparing Intensity of Lymphodepletion Before Adoptive Transfer of Tumor-Infiltrating Lymphocytes for Patients With Metastatic Melanoma
- PMID: 27217459
- PMCID: PMC4981979
- DOI: 10.1200/JCO.2016.66.7220
Randomized, Prospective Evaluation Comparing Intensity of Lymphodepletion Before Adoptive Transfer of Tumor-Infiltrating Lymphocytes for Patients With Metastatic Melanoma
Abstract
Purpose: Adoptive cell transfer, the infusion of large numbers of activated autologous lymphocytes, can mediate objective tumor regression in a majority of patients with metastatic melanoma (52 of 93; 56%). Addition and intensification of total body irradiation (TBI) to the preparative lymphodepleting chemotherapy regimen in sequential trials improved objective partial and complete response (CR) rates. Here, we evaluated the importance of adding TBI to the adoptive transfer of tumor-infiltrating lymphocytes (TIL) in a randomized fashion.
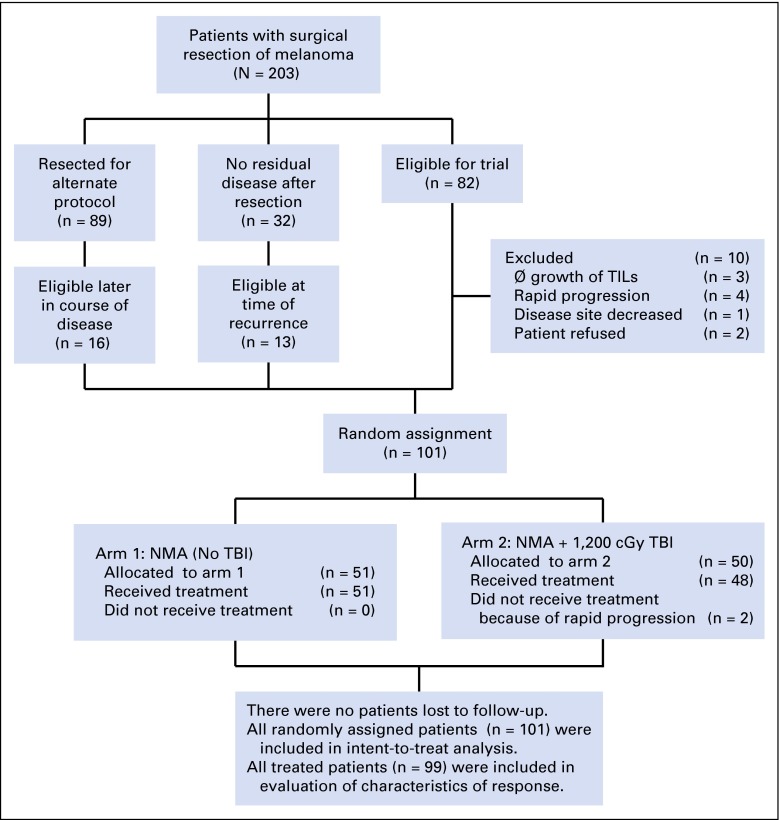
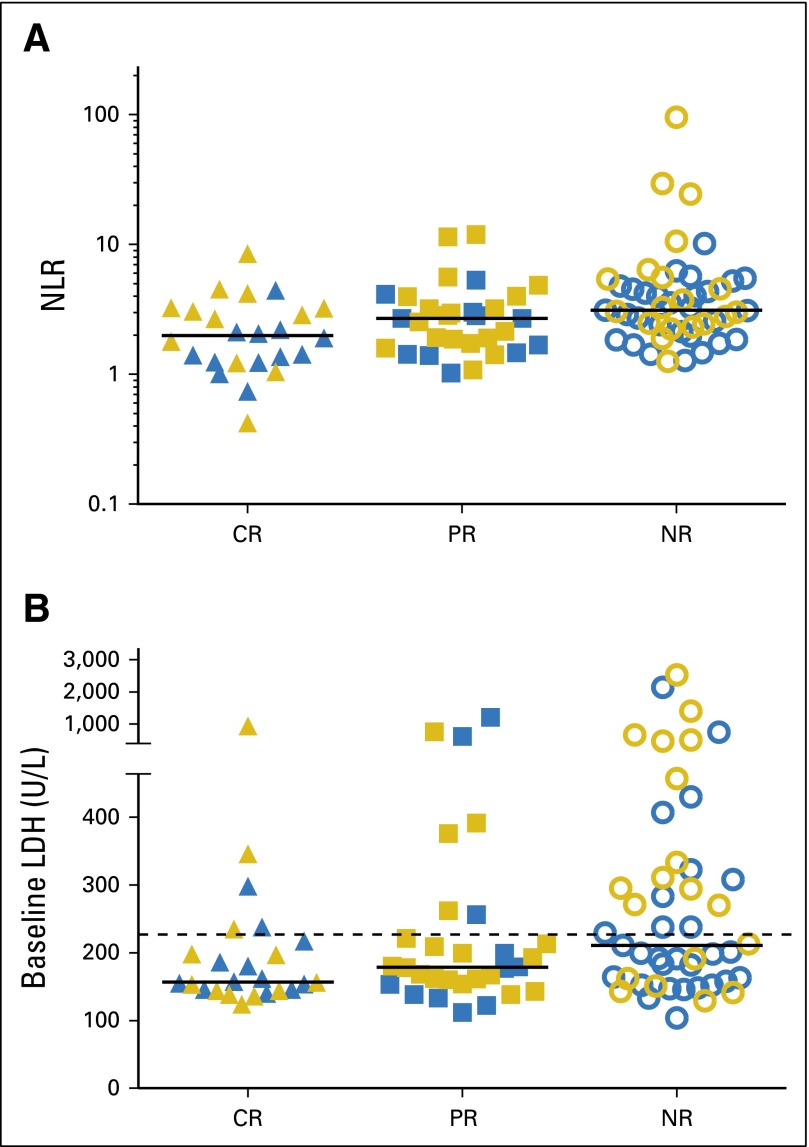
Patients and methods: A total of 101 patients with metastatic melanoma, including 76 patients with M1c disease, were randomly assigned to receive nonmyeloablative chemotherapy with or without 1,200 cGy TBI before transfer of tumor-infiltrating lymphcytes. Primary end points were CR rate (as defined by Response Evaluation Criteria in Solid Tumors v1.0) and overall survival (OS). Clinical and laboratory data were analyzed for correlates of response.
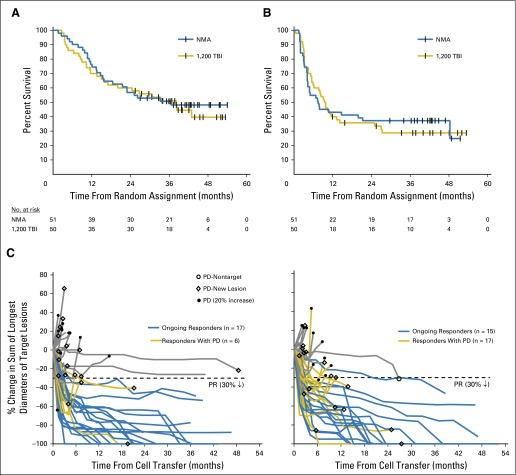
Results: CR rates were 24% in both groups (12 of 50 v 12 of 51), and OS was also similar (median OS, 38.2 v 36.6 months; hazard ratio, 1.11; 95% CI, 0.65 to 1.91; P = .71). Thrombotic microangiopathy was an adverse event unique to the TBI arm and occurred in 13 of 48 treated patients. With a median potential follow-up of 40.9 months, only one of 24 patients who achieved a CR recurred.
Conclusion: Adoptive cell transfer can mediate durable complete regressions in 24% of patients with metastatic melanoma, with median survival > 3 years. Results were similar using chemotherapy preparative regimens with or without addition of TBI.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Melanoma: Improving durable responses with TILs.Nat Rev Clin Oncol. 2016 Jul;13(7):397. doi: 10.1038/nrclinonc.2016.95. Epub 2016 Jun 14. Nat Rev Clin Oncol. 2016. PMID: 27296294 No abstract available.
References
-
- American Cancer Society: Cancer Facts and Figures 2015. Atlanta, GA, American Cancer Society, 2015.
-
- Wingo PA, Tong T, Bolden S. Cancer statistics, 1995. CA Cancer J Clin. 1995;45:8–30. - PubMed
-
- Rosenberg SA, Lotze MT, Muul LM, et al. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med. 1985;313:1485–1492. - PubMed
-
- Rosenberg SA, Yannelli JR, Yang JC, et al. Treatment of patients with metastatic melanoma with autologous tumor-infiltrating lymphocytes and interleukin 2. J Natl Cancer Inst. 1994;86:1159–1166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
