

Atrial Fibrillation Is Associated With a Worse 90-Day Outcome Than Other Cardioembolic Stroke Subtypes
- PMID: 27217503
- PMCID: PMC4880452
- DOI: 10.1161/STROKEAHA.116.012865
Atrial Fibrillation Is Associated With a Worse 90-Day Outcome Than Other Cardioembolic Stroke Subtypes
Abstract
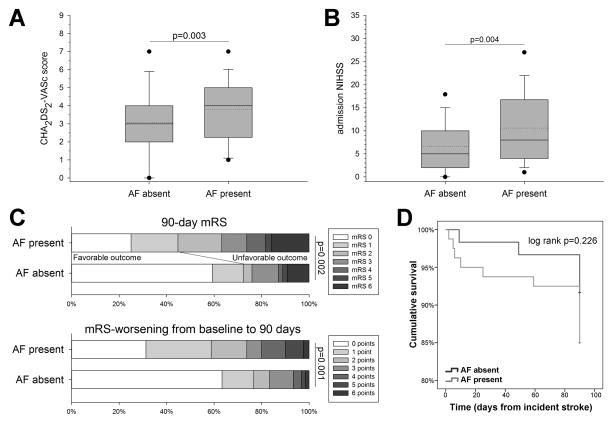
Background and purpose: Patients with a cardioembolic stroke (CES) have worse outcomes than stroke patients with other causes of stroke. Among patients with CES, atrial fibrillation (AF) is a common comorbidity. Mounting data indicate that AF may be related to stroke pathogenesis beyond acute cerebral thromboembolism. We sought to determine whether AF represents an independent risk factor for stroke severity and outcome among patients with CES.
Methods: We retrospectively analyzed patients with acute hemispheric CES included in an academic medical center's stroke registry. CES was determined using the Causative Classification System of ischemic stroke. Multivariable logistic regression was used to determine whether AF was associated with 90-day outcome functional status.
Results: Our cohort included 140 patients. Of these, 52 had prevalent AF and 28 had incident AF diagnosed during their index hospitalization or within 90 days of hospital discharge. After adjustment for potential confounders or mediators, any AF (odds ratio, 2.51; 95% confidence interval, 1.03-6.33; P=0.049), infarct volume (odds ratio, 1.03; 95% confidence interval, 1.01-1.06; P=0.005), preadmission modified Rankin Scale score (odds ratio, 2.58; 95% confidence interval, 1.66-4.01; P<0.001), and admission National Institutes of Health Stroke Scale score (odds ratio, 1.17; 95% confidence interval, 1.08-1.28; P<0.001) remained associated with an unfavorable 90-day outcome (modified Rankin Scale score, 2-6).
Conclusions: AF is associated with an unfavorable 90-day outcome among patients with a CES independent of established risk factors and initial stroke severity. This suggests that AF-specific mechanisms affect CES severity and functional status after CES. If confirmed in future studies, further investigation into the underlying pathophysiological mechanisms may provide novel avenues to AF detection and treatment.
Keywords: atrial fibrillation; cerebral infarction; classification; outcomes research; risk factors; stroke.
© 2016 American Heart Association, Inc.
Figures

References
-
- CDC, NCHS. Underlying Cause of Death 1999–2014 on CDC WONDER Online Database, released 2015. [Accessed April 1, 2015];Data are from the Multiple Cause of Death Files, 1999–2014, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. http://wonder.cdc.gov/ucd-icd10.html.
-
- Lovett JK, Coull AJ, Rothwell PM. Early risk of recurrence by subtype of ischemic stroke in population-based incidence studies. Neurology. 2004;62:569–573. - PubMed
-
- Marnane M, Duggan CA, Sheehan OC, Merwick A, Hannon N, Curtin D, et al. Stroke subtype classification to mechanism-specific and undetermined categories by TOAST, AS-C-O, and causative classification system: direct comparison in the North Dublin population stroke study. Stroke. 2010;41:1579–1586. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
