

A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear production in subjects with dry eye disease
- PMID: 27217719
- PMCID: PMC4862385
- DOI: 10.2147/OPTH.S101716
A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear production in subjects with dry eye disease
Abstract
Background: Dry eye disease (DED), a chronic disorder affecting the tear film and lacrimal functional unit, is a widely prevalent condition associated with significant burden and unmet treatment needs. Since specific neural circuits play an important role in maintaining ocular surface health, microelectrical stimulation of these pathways could present a promising new approach to treating DED. This study evaluated the efficacy and safety of nasal electrical stimulation in patients with DED.
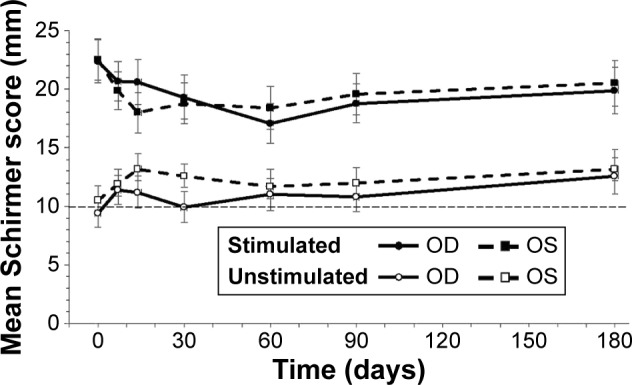
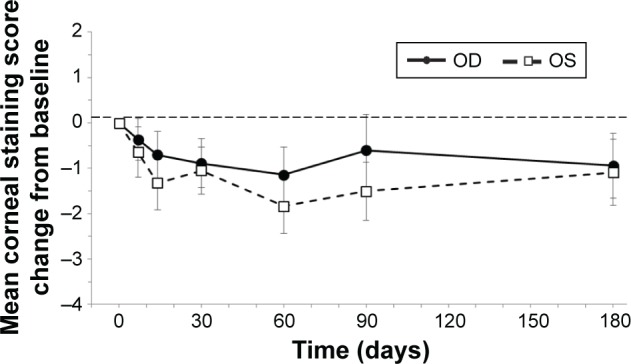
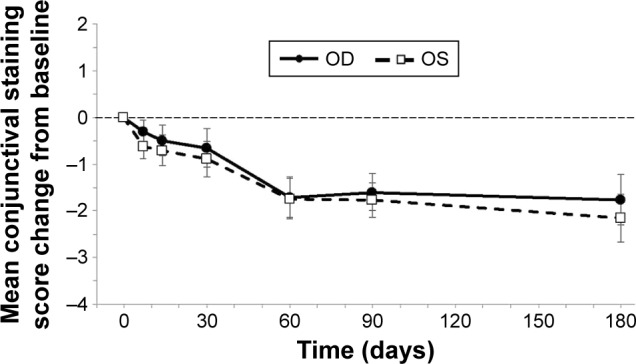
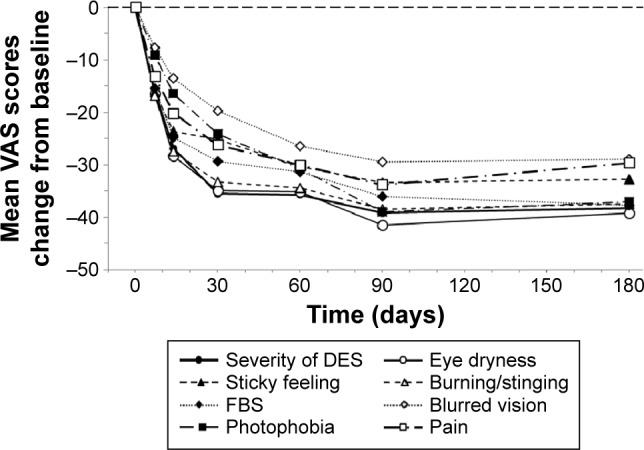
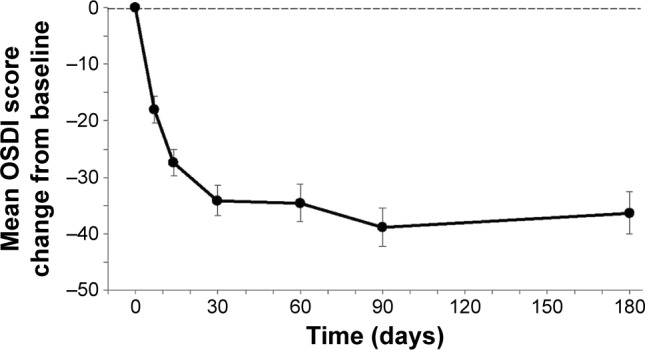
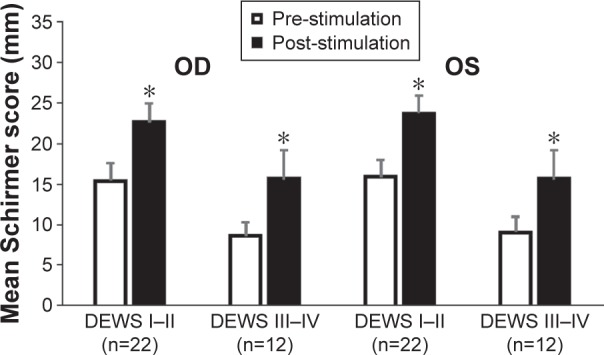
Methods: This prospective, open-label, single-arm, nonrandomized pilot study included 40 patients with mild to severe DED. After undergoing two screening visits, enrolled subjects were provided with a nasal stimulation device and instructed to use it at home four times daily (or more often as needed). Follow-up assessments were conducted up to day 180. The primary efficacy endpoint was the difference between unstimulated and stimulated tear production quantified by Schirmer scores. Additional efficacy endpoints included change from baseline in corneal and conjunctival staining, symptoms evaluated on a Visual Analog Scale, and Ocular Surface Disease Index scores. Safety parameters included adverse event (AE) rates, visual acuity, intraocular pressure, slit-lamp biomicroscopy, indirect ophthalmoscopy, and endoscopic nasal examinations.
Results: Mean stimulated Schirmer scores were significantly higher than the unstimulated scores at all visits, and corneal and conjunctival staining and symptom scores from baseline to day 180 were significantly reduced. No serious device-related AEs and nine nonserious AEs (three device-related) were reported. Intraocular pressure remained stable and most subjects showed little or no change in visual acuity at days 30 and 180. No significant findings from other clinical examinations were noted.
Conclusion: Neurostimulation of the nasolacrimal pathway is a safe and effective means of increasing tear production and reducing symptoms of dry eye in patients with DED.
Keywords: keratoconjunctivitis sicca; nasolacrimal reflex; neuromodulation; neurostimulation; ocular staining; tear production.
Figures
References
-
- The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):75–92. - PubMed
-
- Behrens A, Doyle JJ, Stern L, et al. Dysfunctional Tear Syndrome Study Group Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea. 2006;25(8):900–907. - PubMed
-
- O’Brien PD, Collum LM. Dry eye: diagnosis and current treatment strategies. Curr Allergy Asthma Rep. 2004;4:314–319. - PubMed
-
- Stapleton F, Garrett Q, Chan C, Craig JP. The epidemiology of dry eye disease. In: Chan C, editor. Dry Eye: A Practical Approach. Springer; Berlin: 2015. pp. 21–29.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
