

Sodium Excretion and the Risk of Cardiovascular Disease in Patients With Chronic Kidney Disease
- PMID: 27218629
- PMCID: PMC5087595
- DOI: 10.1001/jama.2016.4447
Sodium Excretion and the Risk of Cardiovascular Disease in Patients With Chronic Kidney Disease
Abstract
Importance: Patients with chronic kidney disease (CKD) are at an increased risk of cardiovascular disease (CVD) compared with the general population. Prior studies have produced contradictory results on the association of dietary sodium intake with risk of CVD, and this relationship has not been investigated in patients with CKD.
Objective: To evaluate the association between urinary sodium excretion and clinical CVD events among patients with CKD.
Design, setting, and participants: A prospective cohort study of patients with CKD from 7 locations in the United States enrolled in the Chronic Renal Insufficiency Cohort Study and followed up from May 2003 to March 2013.
Exposures: The cumulative mean of urinary sodium excretion from three 24-hour urinary measurements and calibrated to sex-specific mean 24-hour urinary creatinine excretion.
Main outcomes and measures: A composite of CVD events defined as congestive heart failure, stroke, or myocardial infarction. Events were reported every 6 months and confirmed by medical record adjudication.
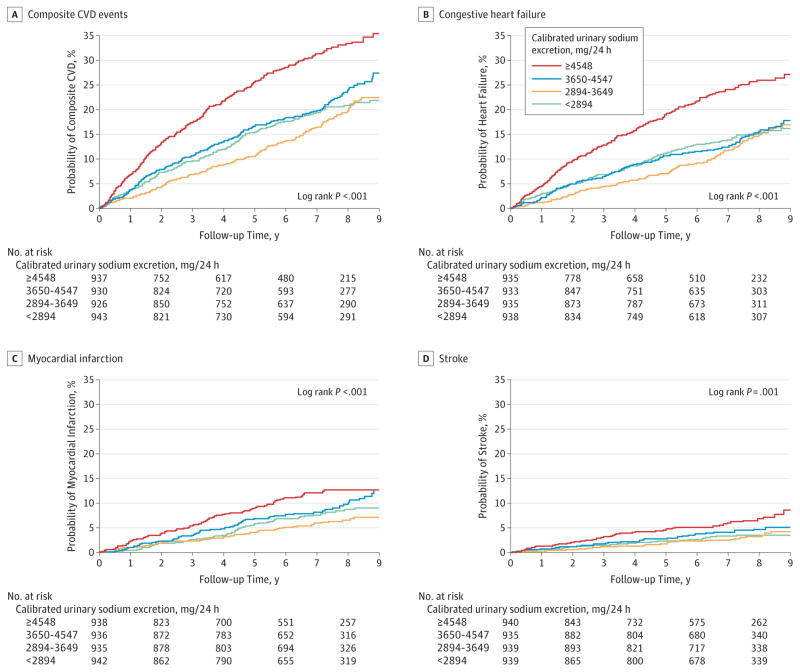
Results: Among 3757 participants (mean age, 58 years; 45% women), 804 composite CVD events (575 heart failure, 305 myocardial infarction, and 148 stroke) occurred during a median 6.8 years of follow-up. From lowest (<2894 mg/24 hours) to highest (≥4548 mg/24 hours) quartile of calibrated sodium excretion, 174, 159, 198, and 273 composite CVD events occurred, and the cumulative incidence was 18.4%, 16.5%, 20.6%, and 29.8% at median follow-up. In addition, the cumulative incidence of CVD events in the highest quartile of calibrated sodium excretion compared with the lowest was 23.2% vs 13.3% for heart failure, 10.9% vs 7.8% for myocardial infarction, and 6.4% vs 2.7% for stroke at median follow-up. Hazard ratios of the highest quartile compared with the lowest quartile were 1.36 (95% CI, 1.09-1.70; P = .007) for composite CVD events, 1.34 (95% CI, 1.03-1.74; P = .03) for heart failure, and 1.81 (95% CI, 1.08-3.02; P = .02) for stroke after multivariable adjustment. Restricted cubic spline analyses of the association between sodium excretion and composite CVD provided no evidence of a nonlinear association (P = .11) and indicated a significant linear association (P < .001).
Conclusions and relevance: Among patients with CKD, higher urinary sodium excretion was associated with increased risk of CVD.
Conflict of interest statement
Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Steigerwalt reported having received support from Medtronic as a principal investigator for 2 trials and travel expenses from ATCOR. Dr Townsend reported having received support from Medtronic, Janssen, Relypsa, and UpToDate. No other disclosures were reported.
Figures

Comment in
-
Dietary Salt, Kidney Disease, and Cardiovascular Health.JAMA. 2016 May 24-31;315(20):2173-4. doi: 10.1001/jama.2016.5985. JAMA. 2016. PMID: 27218627 No abstract available.
-
Sodium Excretion, Cardiovascular Disease, and Chronic Kidney Disease.JAMA. 2016 Sep 13;316(10):1112. doi: 10.1001/jama.2016.11550. JAMA. 2016. PMID: 27623467 No abstract available.
-
Sodium Excretion, Cardiovascular Disease, and Chronic Kidney Disease.JAMA. 2016 Sep 13;316(10):1112. doi: 10.1001/jama.2016.11553. JAMA. 2016. PMID: 27623468 No abstract available.
-
Don't Pass the Salt: Evidence to Support Avoidance of High Salt Intake in CKD.Am J Kidney Dis. 2017 Feb;69(2):175-178. doi: 10.1053/j.ajkd.2016.09.008. Epub 2016 Oct 24. Am J Kidney Dis. 2017. PMID: 27789126 Free PMC article. No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Matsushita K, van der Velde M, Astor BC, et al. Chronic Kidney Disease Prognosis Consortium. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–2081. - PMC - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics: 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. - PubMed
-
- He FJ, Li J, Macgregor GA. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ. 2013;346:f1325. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01DK060963/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U01DK061022/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 RR-024131/RR/NCRR NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR-000424/TR/NCATS NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R01DK074615/DK/NIDDK NIH HHS/United States
- U01DK060980/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- U01DK061021/DK/NIDDK NIH HHS/United States
- U01DK060984/DK/NIDDK NIH HHS/United States
- UL1RR029879/RR/NCRR NIH HHS/United States
- U01DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- U01DK061028/DK/NIDDK NIH HHS/United States
- UL1TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- T32HL007024/HL/NHLBI NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01DK060902/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- M01 RR-16500/RR/NCRR NIH HHS/United States
- K23 DK094829/DK/NIDDK NIH HHS/United States
- R01 DK074615/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
