

Randomised clinical trial: a phase 1, dose-ranging study of the anti-matrix metalloproteinase-9 monoclonal antibody GS-5745 versus placebo for ulcerative colitis
- PMID: 27218676
- PMCID: PMC5089609
- DOI: 10.1111/apt.13653
Randomised clinical trial: a phase 1, dose-ranging study of the anti-matrix metalloproteinase-9 monoclonal antibody GS-5745 versus placebo for ulcerative colitis
Abstract
Background: Matrix metalloproteinase-9 is a proteolytic enzyme whose expression is increased in ulcerative colitis.
Aim: To evaluate the safety and efficacy of GS-5745, a fully humanised anti-matrix metalloproteinase-9 monoclonal antibody, in moderately-to-severely active ulcerative colitis.
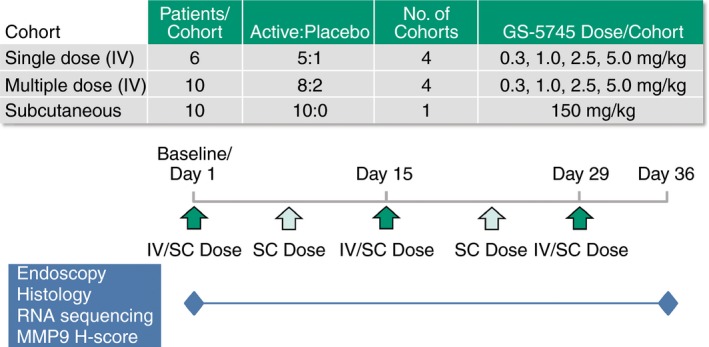
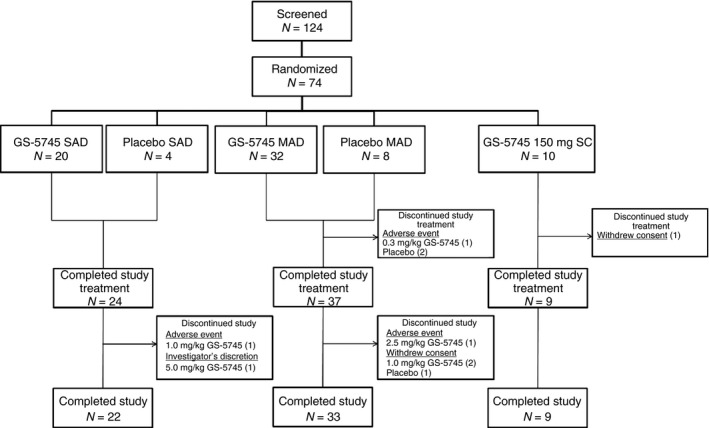
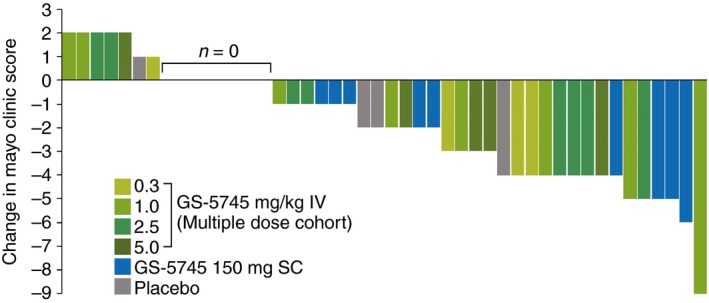
Methods: We randomised 74 patients with ulcerative colitis to treatment with single or multiple ascending intravenous or subcutaneous doses of GS-5745 or placebo. Multiple-dose cohorts received either IV infusions (0.3, 1.0, 2.5 or 5.0 mg/kg GS-5745 or placebo) every 2 weeks (three total IV infusions) or five weekly SC injections (150 mg GS-5745 or placebo). The primary outcomes were the safety, tolerability and pharmacokinetics of escalating single and multiple doses of GS-5745. Exploratory analyses in the multiple-dose cohorts included clinical response (≥3 points or 30% decrease from baseline in Mayo Clinic score and ≥1 point decrease in the rectal bleeding subscore or a rectal bleeding subscore ≤1) and clinical remission (a complete Mayo Clinic score ≤2 with no subscore >1) at Day 36. Biological effects associated with a clinical response to GS-5745 were explored using histological and molecular approaches.
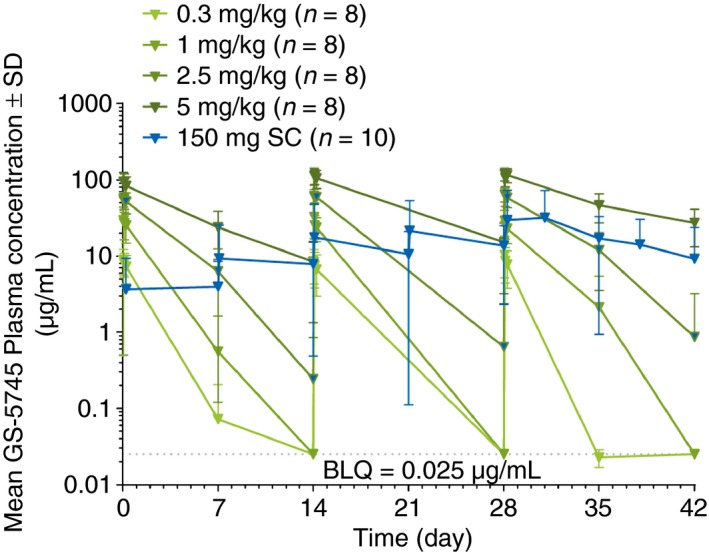
Results: Twenty-three of the 42 patients (55%) receiving multiple doses of GS-5745 had adverse events, compared with 5/8 patients (63%) receiving placebo. GS-5745 showed target-mediated drug disposition, approximately dose-proportional increases in maximum plasma concentration and more than dose-proportional increases in the area under the plasma drug concentration-time curve. Clinical response occurred in 18/42 patients (43%) receiving GS-5745 compared with 1/8 patients (13%) receiving placebo. Clinical remission occurred in 6/42 patients (14%) receiving GS-5745 and 0/8 (0%) receiving placebo. Patients with a clinical response to GS-5745 had reductions in matrix metalloproteinase-9 tissue levels (mean 48.9% decrease from baseline compared with a mean 18.5% increase in nonresponders, P = 0.008) significant improvements in histopathology scores (confirmed with three separate histological disease activity indices), as well as changes in colonic gene expression that were consistent with reduced inflammation.
Conclusion: This phase 1 trial provides preliminary evidence for the safety and therapeutic potential of GS-5745 in the treatment of ulcerative colitis.
© 2016 The Authors. Alimentary Pharmacology & Therapeutics published by John Wiley & Sons Ltd.
Figures
Comment in
-
Letter: anti-matrix metalloproteinase-9 monoclonal antibody GS-5745 for ulcerative colitis.Aliment Pharmacol Ther. 2016 Oct;44(7):767. doi: 10.1111/apt.13735. Aliment Pharmacol Ther. 2016. PMID: 27593425 No abstract available.
References
-
- Ordás I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet 2012; 380: 1606–19. - PubMed
-
- Kornbluth A, Sachar DB; Practice Parameters Committee of the American College of Gastroenterology . Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 2010; 105: 501–23. - PubMed
-
- Feagan BG, Rutgeerts P, Sands BE, et al Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med 2013; 369: 699–710. - PubMed
-
- Allez M, Karmiris K, Louis E, et al Report of the ECCO pathogenesis workshop on anti‐TNF therapy failures in inflammatory bowel diseases: definitions, frequency and pharmacological aspects. J Crohns Colitis 2010; 4: 355–66. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical