

The Burden of Cryptosporidium Diarrheal Disease among Children < 24 Months of Age in Moderate/High Mortality Regions of Sub-Saharan Africa and South Asia, Utilizing Data from the Global Enteric Multicenter Study (GEMS)
- PMID: 27219054
- PMCID: PMC4878811
- DOI: 10.1371/journal.pntd.0004729
The Burden of Cryptosporidium Diarrheal Disease among Children < 24 Months of Age in Moderate/High Mortality Regions of Sub-Saharan Africa and South Asia, Utilizing Data from the Global Enteric Multicenter Study (GEMS)
Abstract
Background: The importance of Cryptosporidium as a pediatric enteropathogen in developing countries is recognized.
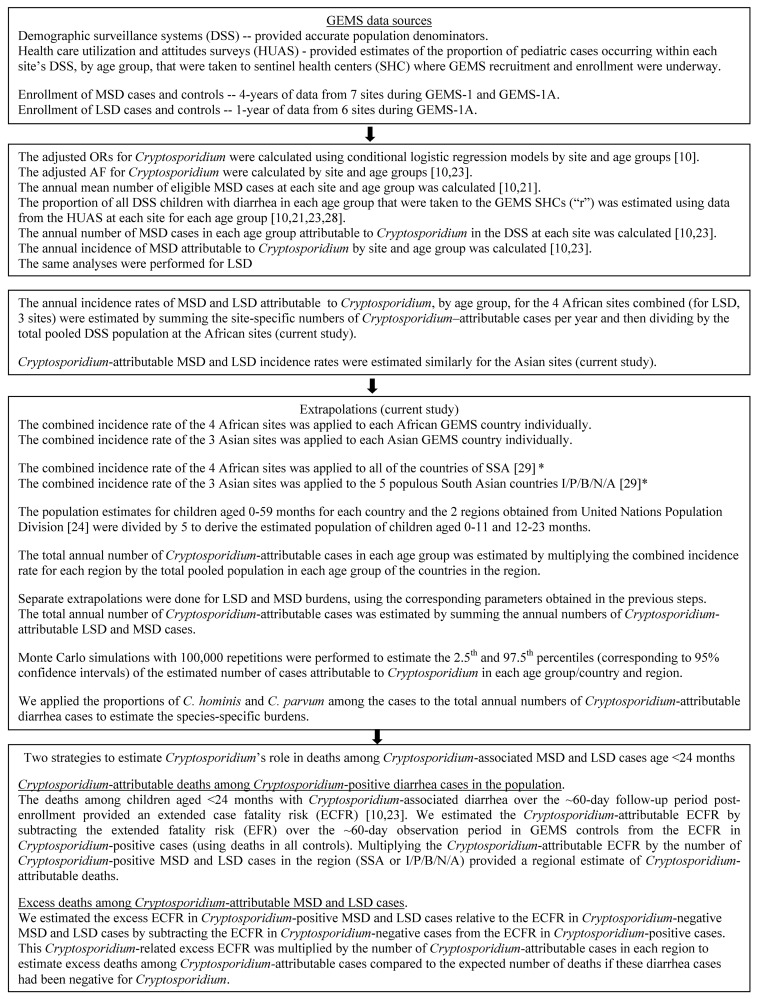
Methods: Data from the Global Enteric Multicenter Study (GEMS), a 3-year, 7-site, case-control study of moderate-to-severe diarrhea (MSD) and GEMS-1A (1-year study of MSD and less-severe diarrhea [LSD]) were analyzed. Stools from 12,110 MSD and 3,174 LSD cases among children aged <60 months and from 21,527 randomly-selected controls matched by age, sex and community were immunoassay-tested for Cryptosporidium. Species of a subset of Cryptosporidium-positive specimens were identified by PCR; GP60 sequencing identified anthroponotic C. parvum. Combined annual Cryptosporidium-attributable diarrhea incidences among children aged <24 months for African and Asian GEMS sites were extrapolated to sub-Saharan Africa and South Asian regions to estimate region-wide MSD and LSD burdens. Attributable and excess mortality due to Cryptosporidium diarrhea were estimated.
Findings: Cryptosporidium was significantly associated with MSD and LSD below age 24 months. Among Cryptosporidium-positive MSD cases, C. hominis was detected in 77.8% (95% CI, 73.0%-81.9%) and C. parvum in 9.9% (95% CI, 7.1%-13.6%); 92% of C. parvum tested were anthroponotic genotypes. Annual Cryptosporidium-attributable MSD incidence was 3.48 (95% CI, 2.27-4.67) and 3.18 (95% CI, 1.85-4.52) per 100 child-years in African and Asian infants, respectively, and 1.41 (95% CI, 0.73-2.08) and 1.36 (95% CI, 0.66-2.05) per 100 child-years in toddlers. Corresponding Cryptosporidium-attributable LSD incidences per 100 child-years were 2.52 (95% CI, 0.33-5.01) and 4.88 (95% CI, 0.82-8.92) in infants and 4.04 (95% CI, 0.56-7.51) and 4.71 (95% CI, 0.24-9.18) in toddlers. We estimate 2.9 and 4.7 million Cryptosporidium-attributable cases annually in children aged <24 months in the sub-Saharan Africa and India/Pakistan/Bangladesh/Nepal/Afghanistan regions, respectively, and ~202,000 Cryptosporidium-attributable deaths (regions combined). ~59,000 excess deaths occurred among Cryptosporidium-attributable diarrhea cases over expected if cases had been Cryptosporidium-negative.
Conclusions: The enormous African/Asian Cryptosporidium disease burden warrants investments to develop vaccines, diagnostics and therapies.
Conflict of interest statement
Three authors are affiliated with companies. YW is a biostatistician who presently works for Emergent Biosolutions, Gaithersburg, M; DSah is Senior Manager, Epidemiology, at GSK Vaccines, Wavre, Belgium; RA is Global Director, Scientific Affairs at GSK Vaccines, Wavre, Belgium. In each instance these individuals took those positions after having completed their participation in the GEMS project and their current work does not involve research on Cryptosporidium vaccines. SMT and MML are co-investigators on a NIH grant that involves upstream basic research towards the development of a candidate vaccine to prevent disease caused by Cryptosporidium hominis. No other authors have relevant declarations relating to employment, consultancy, patents, products in development or marketed products related to Cryptosporidium.
Figures
References
-
- Chappell CL, Okhuysen PC. Cryptosporidiosis. Curr Opin Infect Dis 2002. October;15(5):523–7. - PubMed
-
- Snelling WJ, Xiao L, Ortega-Pierres G, Lowery CJ, Moore JE, Rao JR, et al. Cryptosporidiosis in developing countries. J Infect Dev Ctries 2007. December 1;1(3):242–56. - PubMed
-
- Mac Kenzie WR, Hoxie NJ, Proctor ME, Gradus MS, Blair KA, Peterson DE, et al. A massive outbreak in Milwaukee of cryptosporidium infection transmitted through the public water supply. N Engl J Med 1994. July 21;331(3):161–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
