

Magnesium nebulization utilization in management of pediatric asthma (MagNUM PA) trial: study protocol for a randomized controlled trial
- PMID: 27220675
- PMCID: PMC4879727
- DOI: 10.1186/s13063-015-1151-x
Magnesium nebulization utilization in management of pediatric asthma (MagNUM PA) trial: study protocol for a randomized controlled trial
Abstract
Background: Up to 30 % of children with acute asthma are refractory to initial therapy, and 84 % of this subpopulation needs hospitalization. Finding safe, noninvasive, and effective strategies to treat this high-risk group would substantially decrease hospitalizations, healthcare costs, and the psycho-social burden of the disease. Whereas intravenous magnesium (Mg) is effective in severe refractory asthma, its use is sporadic due to safety concerns, with the main treatment goal being to prevent intensive care unit admission. In contrast, nebulized Mg is noninvasive, allows higher pulmonary drug concentrations, and has a much higher safety potential due to the lower rate of systemic delivery. Previous studies of inhaled Mg show disparate results due to the use of unknown/inefficient delivery methods and other methodological flaws.
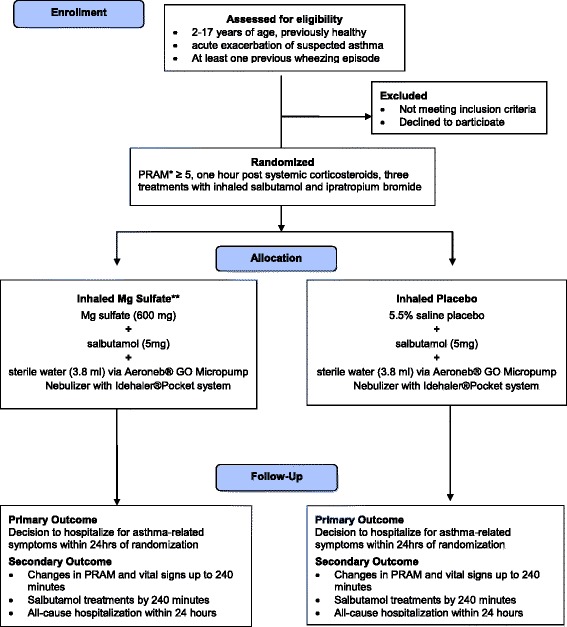
Methods/design: The study is a randomized double-blind controlled trial in seven Canadian pediatric Emergency Departments (two-center pilot 2011 to 2014, Canada-wide November 2014 to December 2017). The trial will include 816 otherwise healthy children who are 2 to 17 years old, having had at least one previous wheezing episode, have received systemic corticosteroids, and have a Pediatric Respiratory Assessment Measure (PRAM) ≥ 5 points after three salbutamol and ipratropium treatments for a current acute asthma exacerbation. Eligible consenting children will receive three experimental treatments of nebulized salbutamol with either 600 mg of Mg sulfate or placebo 20 min apart, using an Aeroneb Go nebulizer, which has been shown to maximize pulmonary delivery while maintaining safety. The primary outcome is hospitalization within 24 h of the start of the experimental therapy for persistent respiratory distress or supplemental oxygen. Secondary outcomes include all-cause hospitalization within 24 h, PRAM, vital signs, number of bronchodilator treatments by 240 min, and the association between the difference in the primary outcome between the groups, age, gender, baseline PRAM, atopy, and "viral induced wheeze" phenotype (Fig. 1).
Discussion: If effective, inhaled Mg may represent an effective strategy to minimize morbidity in pediatric refractory acute asthma. Unlike previous works, this trial targets nonresponders to optimized initial therapy who are the most likely to benefit from inhaled Mg. Future dissemination of results will include knowledge translation, incorporation into a Cochrane Review, presentation at scientific meetings, and a peer-reviewed publication.
Trial registration: NCTO1429415 , registered 2 September 2011.
Trial registration: ClinicalTrials.gov NCT01429415.
Keywords: Randomized controlled trial; acute asthma; children; magnesium.
Figures
References
-
- Mannino DM, Homa DM, Pertowski CA, Ashizawa A, Nixon LL, Johnson CA, et al. Surveillance for asthma–United States, 1960–1995. MMWR CDC Surveill Summ. 1998;47:1–27. - PubMed
-
- Akinbami L. Asthma prevalence, health care use and mortality: United States, 2003–2005. November: Centers for Disease Control and Prevention; 2006. http://www.cdc.gov/nchs/data/hestat/asthma03-05/asthma03-05.htm. Accessed 19 Jan 2016.
-
- Moorman JE, Rudd RA, Johnson CA, King M, Minor P, Bailey C, et al. National surveillance for asthma–United States, 1980–2004. MMWR Surveill Summ. 2007;56:1–54. - PubMed
-
- National Heart, Lung and Blood Institute . Global Initiative for asthma. Global strategy for asthma management and prevention. NHLBI/WHO workshop report. Bethesda, Md: NIH; 2002.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
