

Case Reports
doi: 10.1503/cmaj.151311.
Epub 2016 May 24.
Emergency management of autonomic dysreflexia with neurologic complications
Affiliations
- PMID: 27221275
- PMCID: PMC5056874
- DOI: 10.1503/cmaj.151311
Item in Clipboard
Case Reports
Emergency management of autonomic dysreflexia with neurologic complications
CMAJ.
.
No abstract available
Figures
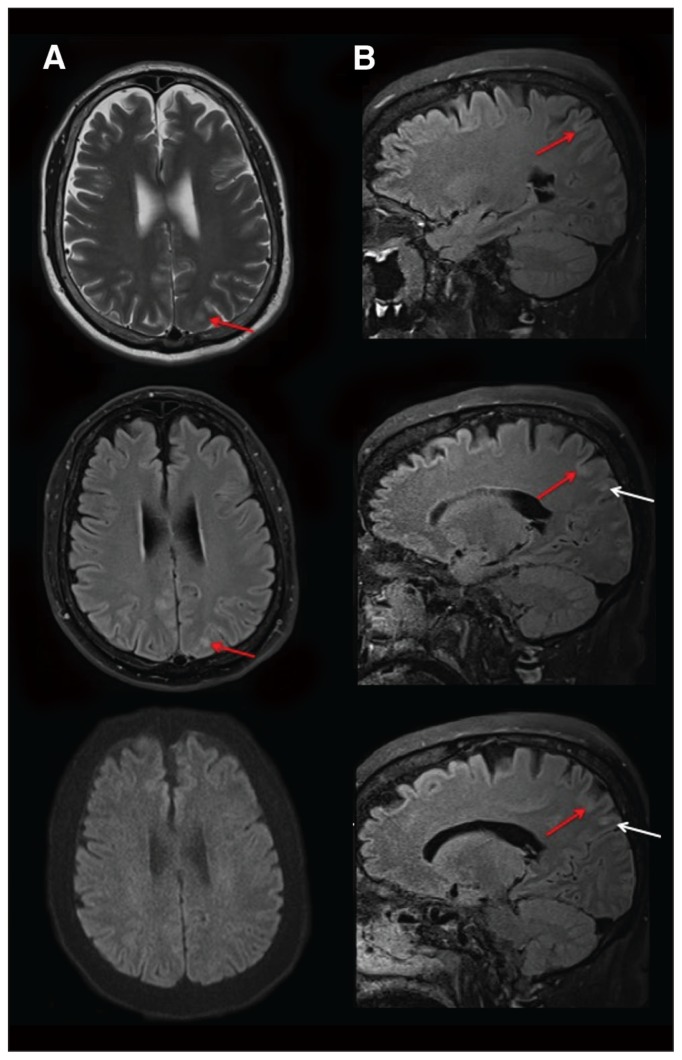
Magnetic resonance imaging consistent with posterior reversible encephalopathy syndrome. (A) Transverse imaging (T2, top; fluid-attenuated inversion recovery, middle; and diffusion-weighted imaging, bottom) shows cortical edema in the left parietal lobe (red arrows). The normal findings on diffusion-weighted imaging (bottom) suggest vasogenic rather than cytotoxic edema. (B) Contiguous sagittal fluid-attenuated inversion recovery images confirmed vasogenic edema in cortical (red arrows) and subcortical (white arrows) areas. Further areas of cortical and subcortical edema were present throughout the parietal and occipital lobes bilaterally (not shown). Given the patient’s acute, severe hypertension, the imaging findings were consistent with mild but evolving posterior reversible encephalopathy syndrome.
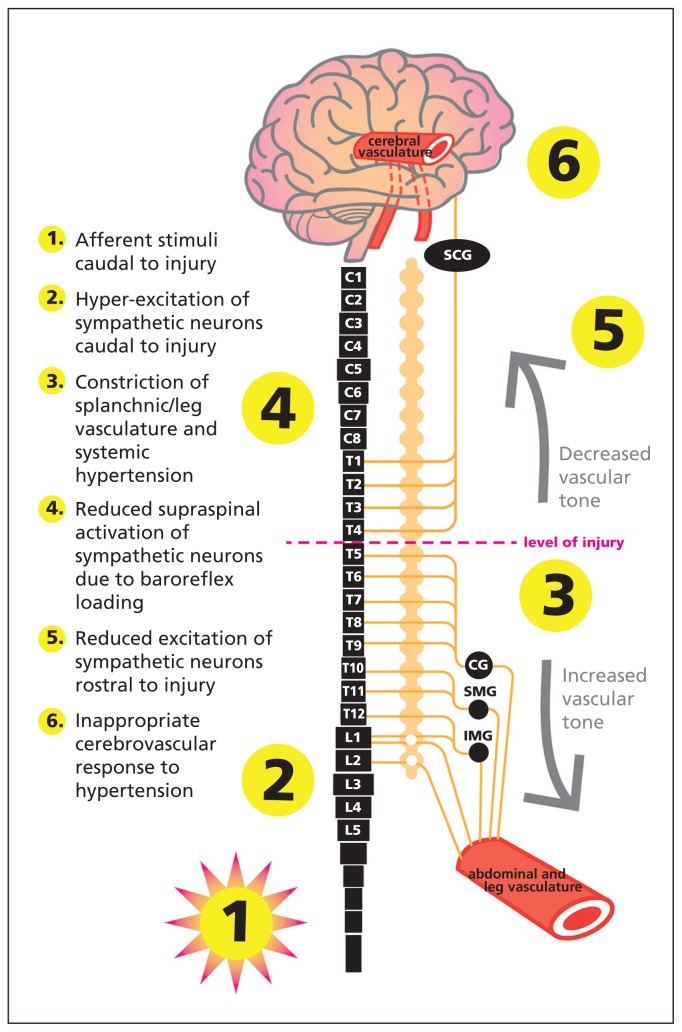
Theoretical framework underlying cerebrovascular events induced by autonomic dysreflexia. In this case, the level of the patient’s injury may have played a role in the development of autonomic dysreflexia–induced posterior reversible encephalopathy syndrome. Specifically, hyperexcitation of the sympathetic preganglionic neurons below the level of injury and a subsequent increase in blood pressure would result in dilatation of the cerebral blood vessels because of intact supraspinal regulation of the superior cervical ganglion (SCG). Paradoxic baroreflex-mediated relaxation of the cerebral arteries would impair autoregulation of the increasing blood pressure and expose the delicate cerebral microvasculature to insulting elevation in cerebral blood flow, potentially compromising the integrity of the blood–brain barrier. CG = celiac ganglion, IMG = inferior mesenteric ganglion, SMG = superior mesenteric ganglion.
References
-
- Phillips AA, Krassioukov AV. Contemporary cardiovascular concerns after spinal cord injury: mechanisms, maladaptations and management. J Neurotrauma 2015;32:1927–42. - PubMed
-
- Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996;334:494–500. - PubMed
-
- Consortium for Spinal Cord Medicine. Acute management of autonomic dysreflexia: individuals with spinal cord injury presenting to health-care facilities. J Spinal Cord Med 2002;25 Suppl 1:S67–88. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical